
Abstract
Abstract
Introduction
G
Several questions have arisen regarding the histologic nature, optimal management, and role and associated risks of preoperative and/or intraoperative drainage.
This article presents 5 case reports of patients treated for giant cysts of the ovary and discusses their pathogenesis, clinical presentation, and management.
Materials and Methods
This was a retrospective descriptive study of 5 cases from the Department of Surgery at Ouakam Military Hospital, in Dakar, Senegal, between January 2009 and December 2012. Patients with large ovarian cysts extending to the epigastric region were selected. Solid, mixed, or predominantly solid ovarian cysts were excluded from the study. Patient assessment included clinical examination, and abdominopelvic ultrasound and computed tomography (CT) scans. Laboratory tests performed were CA-125 and/or ß–human chorionic gonadotropin. Cardiovascular and respiratory anesthetic risk assessments were performed preoperatively. Open surgery (annexectomy) with removal of the cysts was the adopted approach in all the cases.
Results
The 5 patients were in their early reproductive years, with a mean age of 28 (extremes of 22 and 39 years, respectively). Two patients were nulliparous, while the other 3 were multiparous.
Increased abdominal girth accompanied by a sensation of heaviness in the lower abdomen associated with weight gain was present in all cases. Amenorrhea was present in 3 patients. Constipation was noted in 4 cases. Abdominal examination suggested ascites or pseudoascites with abdominal distension and shifting dullness in all cases. A transabdominal fluid thrill was noted without a palpable mass (both liver and spleen were impalpable in each case).
The clinical and laboratory data for all of the patients are summarized in Table 1 and illustrated in figures 1, 2, 3, 4A, 5A,B.
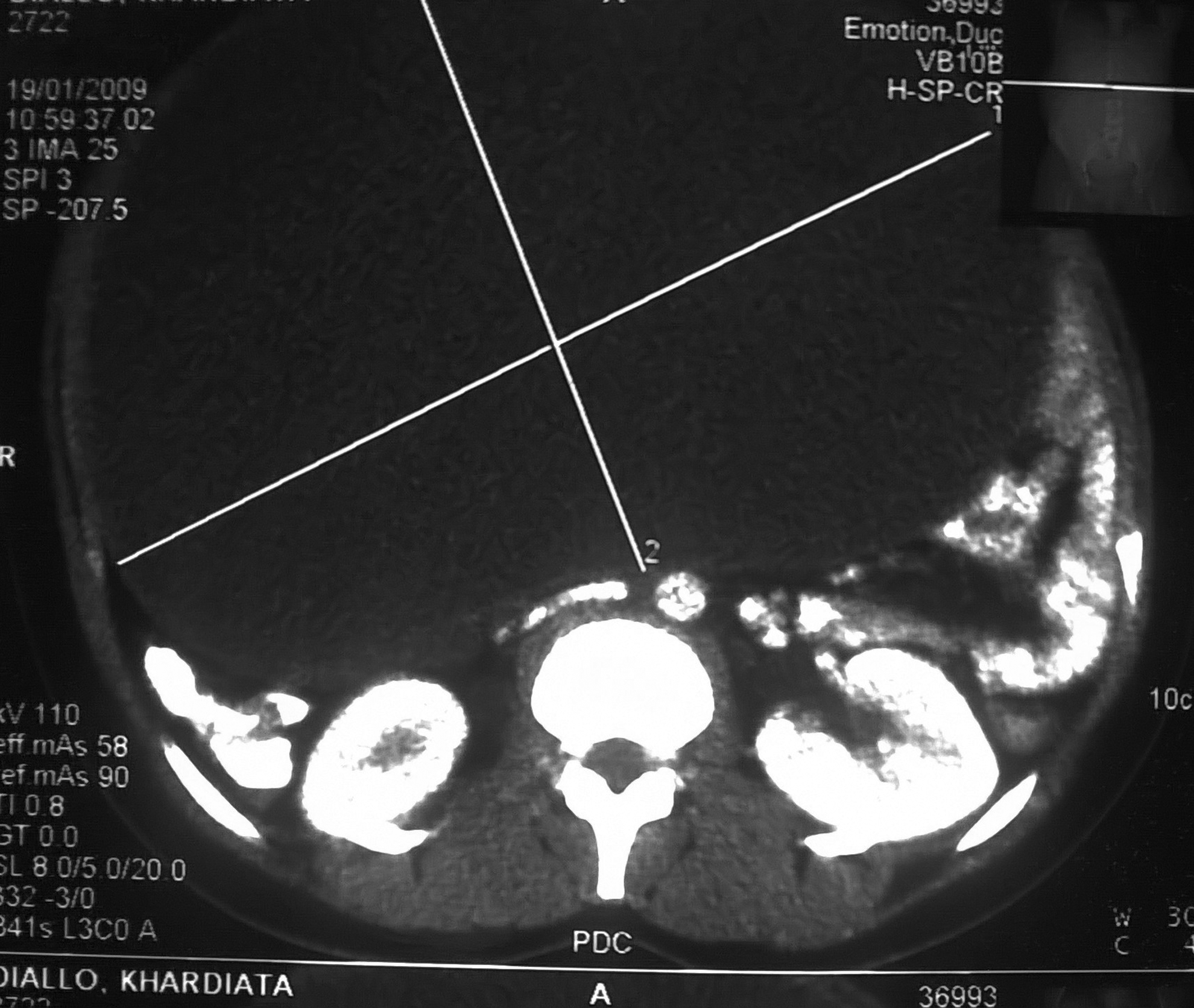
Giant ovarian unilocular cyst reaching epigastric area.

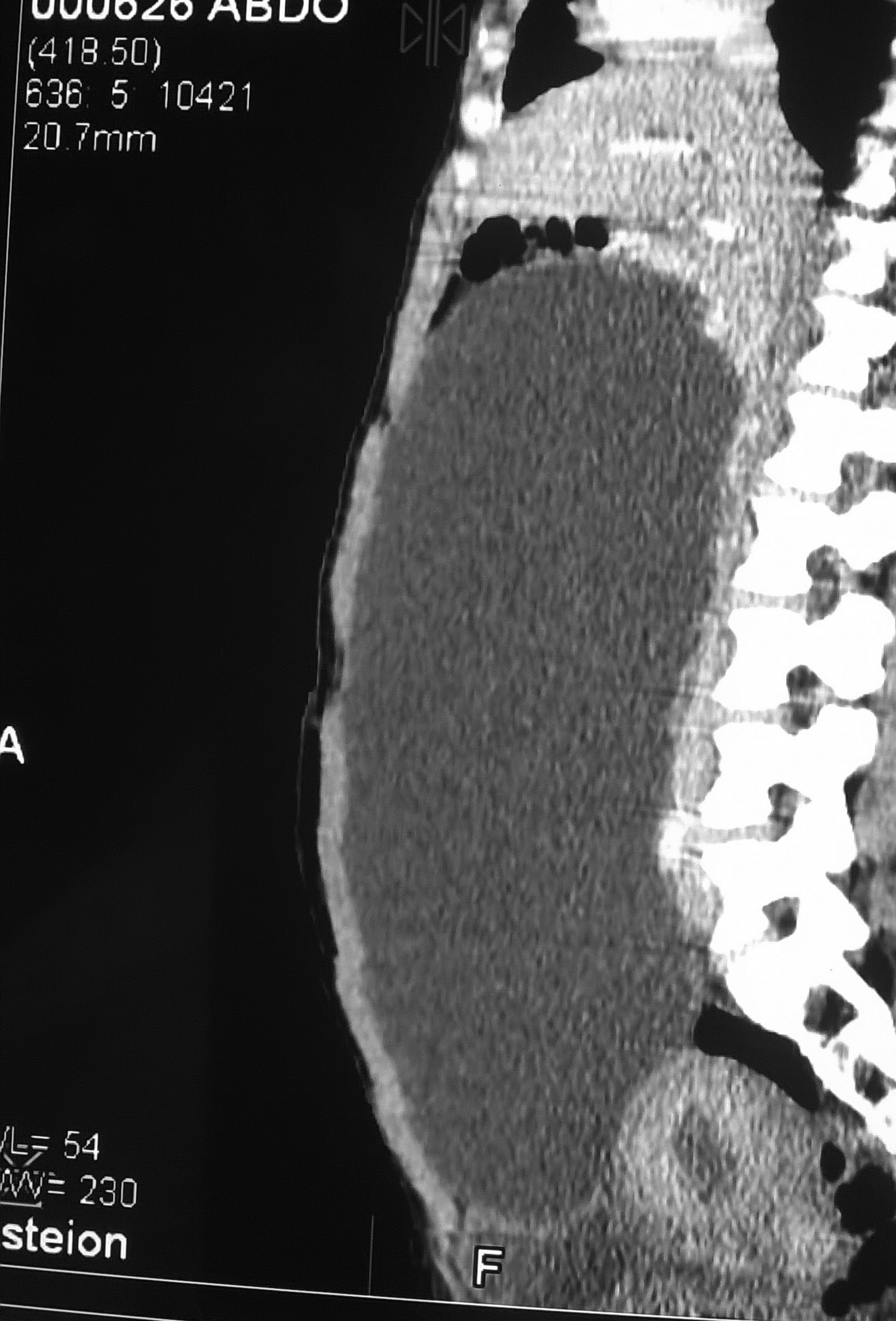
Voluminous abdominal unilocular cyst reaching the epigastric area.

Abdominopelvic unilocular cyst, driving back loops.

Abdominal distension
CT, computed tomography; hCG, human chorionic gonadotropin.
Patient #1 presented with progressive abdominal distension, constipation, and 3 months of amenorrhea. Ultrasound and abdominal CT scans showed a giant, unilocular, thin-walled ovarian cyst without vegetations (Fig. 1). In the month preceding this patient's operation, she noticed a sudden decline in abdominal girth accompanied by polyuria. Her abdominal distension was noted to be less prominent at a review the day prior to surgery, and laparotomy consequently showed a regressed cyst. An enlarged right ovary was noted, with an opaque appearance and a thin film of ascites.
Patient #2 presented with a giant multilocular cyst with minimal ascites. The walls and partitions of the cyst were thick without vegetations (Fig. 2).
Table 2 summarizes intraoperative findings, procedures performed, and histopathology results for all 5 patients. An operative illustration is shown in figure 4B.
See Figure 4B.
Paracentesis or preoperative drainage was not approved by the whole team and was therefore not performed.
The postoperative period was uneventful in all patients. Patients were monitored every 3 months. The average follow-up time was 54 months. No recurrences were observed.
Discussion
Ovarian cysts are benign in 70% of cases and can be fluid-filled, solid, or mixed. The main subtypes are mucinous, serous, endometrioid, and teratoma.1–3 Ovarian cysts may be borderline in 5%–10% of cases and malignant in 20%–25% of cases, largely depending on the age of the patient. 1 These cysts are much more common in young patients of childbearing age—as noted in the current series—and are rare before puberty or after menopause.
Voluminous forms are predominantly serous cystadenomas (75% of cases) and mucinous cysts (25% of cases), sometimes appearing up to impressive dimensions.4,5 Mucinous cystadenomas are benign in 75% of cases, borderline in 10% of cases, and malignant (cystadenocarcinoma) in 15% of cases. This spectrum presents a management dilemma–whether to perform intraoperative laparoscopic-controlled drainage or laparotomy. 6
Giant ovarian cysts, however, are defined differently in the literature. Definitions for giant cysts range from cysts >10 cm seen on imaging studies7,8 to cysts that extend above the umbilicus noted on inspection and abdominal palpation.9,10 These definitions, however, do not include the clinical presentation caused by certain extra-large cysts occupying much of the abdominal cavity up to the diaphragm, as was noted in most of the current patients. These giant ovarian cysts are associated with uncomfortable abdominal distension, heaviness, weight gain, difficulty with walking, discomfort when recumbent, dyspnea or orthopnea, and tachycardia.11,12 Giant cysts, as reported in the literature, might compress the inferior vena cava causing lower- limb edema, compression of the diaphragm with risks of atelectasis, pulmonary edema, and more seriously, abdominal compartment syndrome.1,11,13 In 1905 Spohn reported a 328 pound ovarian tumor. 14 Since then, Abe et al. identified 22 cases of ovarian tumors reported in the literature measuring between 47 kg and 134 kg. 11 The cysts were benign in 72.7% of cases and borderline or malignant in 27.2% of cases.11,15 In a literature review, Einenkel et al. found an overall malignancy rate of 37% in giant ovarian cysts. 12
The differential diagnosis can be difficult to establish in the presence of abundant ascites. Abdominal distension, shifting fluid dullness, and transabdominal fluid thrill were positive findings in all 5 of the current patients, suggesting significant ascites. This demonstrates the difficulty in differentiating ascites from pseudoascites clinically, as many conditions—such as extreme bladder distension, duodenal diverticula, hydronephrosis, mesenteric cysts, cystic echinoccosis, pancreatic pseudocysts, and ovarian cysts—may mimic ascites.16,17
Paracentesis in these settings carries increased peritoneal risks and complications.18,19 Imaging studies (ultrasound, CT scanning, and/or magnetic resonance imaging [MRI]), therefore, are important for establishing the diagnosis and, in addition, may reveal additional findings, such as the presence of a displaced bowel, fluid levels, or a pseudocyst with clear borders (sometimes with endocystic partitions and vegetations).
Preoperative drainage remains controversial. Advantages include reduction of the cyst size, thereby making it easier to manipulate during the operation and extraction, with minimal sacrifice of the parietal wall, and symptomatic relief (reducing intra-abdominal pressure). Similarly, this drainage improves respiratory and cardiovascular function and might prevent pulmonary edema.1,20 Thus, drainage remains relevant for some symptomatic giant cysts. However, it must be performed gradually, with the aim of avoiding long drainage tubes that carry risks of infection, peritonitis, and sudden massive bleeding. 11
The major drawback of drainage however, is the potential dissemination into the peritoneal cavity of a peritoneal carcinoma or gelatinous disease of the peritoneum caused by rupture of a mucinous cyst. 12 Several studies have shown a 10%–26% rate of cyst rupture in cases of laparotomy and 22%–100% for a laparoscopic incision. 3 The lack of quality data on the risk of peritoneal contamination has led some researchers to discourage preoperative drainage. 12 A low-grade mucinous cyst/adenocarcinoma with minimal ascites was noted in the current series. In this case (patient #2), there was no recurrence after 5½ years of follow-up. Other complications are associated with drainage, such as hypovolemic shock, massive hemorrhage, peritonitis, pulmonary edema, pneumonia or atelectasis. 11
Intraoperative laparoscopic-controlled drainage remains as an alternative to laparotomy. It reduces leakage and allows easier removal of the mass.3,7
Conclusions
Extra-large forms of ovarian cysts—while now rare—are a challenge for practitioners. Imaging (ultrasound, CT, and/or MRI) enables the exclusion of ascites, analysis of the cystic wall, and detection of partitions and endo- or exocystic vegetations, which are suspicious features of malignancy. While complete excision without opening the cyst is the procedure of choice, there are minimal data showing the poor outcome of giant cysts that were complicated by rupture or that were drained pre- or intraoperatively.
Footnotes
Acknowledgments
The authors thank Roslyn Mackenzie, MD, for helpful criticism, advice, and assistance with revising and translating the manuscript for this article.
Author Disclosure Statement
The authors report no conflicts of interest.