
Abstract
Abstract
Introduction
D
DIE of the large bowel can be responsible for very severe symptoms, including cramps, constipation, diarrhea, and alternation of constipation and diarrhea. 3 It has also been demonstrated that dysmenorrhea is maximal in cases of infiltration of the vagina and the digestive tract. 4
When there is a symptomatic lesion of the large bowel, resection is often required because of some characteristics of the lesion, such as narrowing of the lumen, large-bowel distortion (Figs. 1 and 2), and fibrosis and nerve infiltration that usually do not respond to medical treatment.1,5 The most frequent large-bowel endometriotic localizations are in the rectum or rectosigmoid junction, followed by the sigmoid colon and the cecum.3,6,7 When there is a severe sigmoid lesion, a segmental sigmoid resection is generally performed.3,6,7 A partial resection of the cecum or an ileocecal resection are the surgical options for addressing ileocecal involvement. For rectal and rectosigmoid junction lesions, three surgical approaches are generally used: (1) colorectal resection removing the affected segment; (2) nodule excision without opening the rectum (shaving); (3) or removal of the nodule along with the surrounding rectal wall (full thickness or discoid excision).6,8
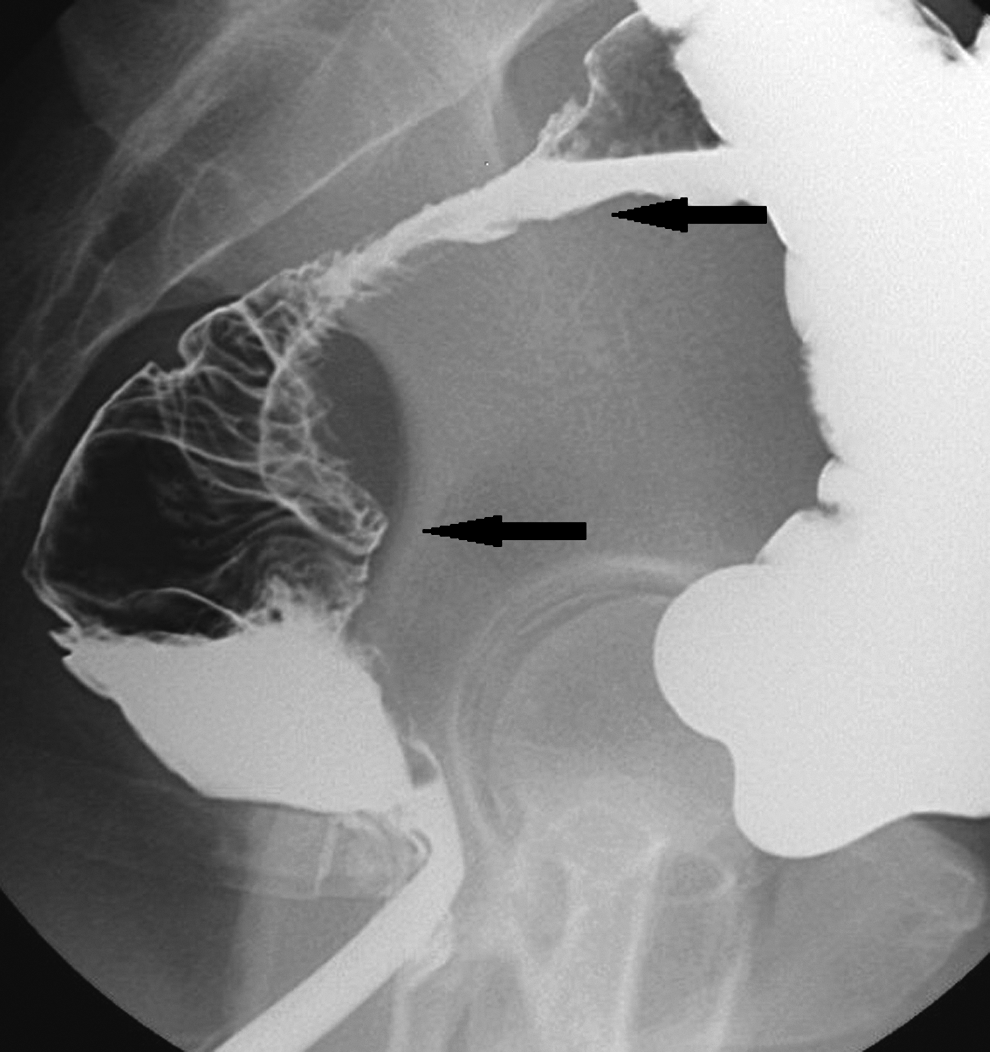
Profile double-contrast barium enema showing severe rectal and rectosigmoid involvement by endometriosis. Arrows show the top and bottom of the colonic involvement with endometriosis.

Magnetic resonance imaging showing severe rectosigmoid endometriosis. Arrow shows endometriotic involvement of the rectosigmoid junction.
The type of treatment (discoid resection versus segmental bowel resection) remains a subject of controversy, and comparative randomized studies must be performed to clarify which type of surgery is superior. DIE can be responsible for very severe complications. Anastomotic leaks and rectovaginal fistulae are the most feared complications.7–9
Other complications have also been reported, such as postoperative abscesses; pre- or postoperative bleeding; voiding dysfunction; urinary retention; ureterovaginal fistulae; sexual disturbances, such as anorgasmia; parietal infections; anal bleeding; dyschezia; and pain on defecation.10–12 Large-bowel endometriosis is a benign condition affecting women of reproductive age almost exclusively. Therefore, the problem of functional complications after colonic or rectal resections and anastomosis is a crucial issue.
The purpose of this research was to study the different aspects of anastomotic stricture (AS) after large-bowel resection and anastomosis for DIE. This study did not concern patients who had “shaving” or partial resection of the rectal anterior wall. The study was approved by the current authors' local ethical committee.
Materials and Methods
Patients' characteristics
Between December 1998 and December 2011, 2535 consecutive patients had surgery for endometriosis. The indication for surgery was pain and/or infertility. Of these patients, 110 (n = 4%; mean age: 33 years ± 6 months) underwent large-bowel resection (resection of the segment of the large bowel affected by DIE and anastomosis of the unaffected proximal and distal sections) for severe symptomatic large-bowel DIE (Figs. 1 and 2). The indication for large-bowel resection was the presence of severe digestive symptoms associated with a suspicion of involvement of the large bowel by DIE as shown on magnetic resonance imaging and double-contrast barium enema (Figs. 1 and 2). A total of 113 colonic resections were performed (3 patients had two resections: rectosigmoid and ileocecal). All 110 patients underwent eradication of all other visible endometriotic lesions.
Large-bowel resection and anastomosis
Among the 110 patients who underwent large-bowel resection, a total of 113 large-bowel resections were performed, including: 31 high resections (located more than 10 cm from the anal verge; including 3 ileocecal resections); 79 low resections (located between 5 and 10 cm from the anal verge); and 3 very-low resections (located <5 cm from the anal verge) were performed (Table 1).
Mean diameters of the strictures are expressed as means ± standard deviation.
AS, anastomotic stricture; EEA, end-to-end anastomosis.
The surgical techniques used (Table 1) were laparoscopically assisted large-bowel resections and anastomosis (87%) as previously described in the literature 13 or laparotomy (13%). These surgical techniques did not vary over the course of 13 years.
Sixty-five patients (59%) who underwent low or very-low resections each had a posterior colpectomy during the same procedure because of the presence of full-thickness posterior vaginal-wall involvement (presence of a dark-bluish induration in the posterior fornix involving the whole vaginal wall and the anterior rectum or rectosigmoid junction; Fig. 2).
The omentum was interposed between the rectal and the vaginal sutures in 48 patients (44%). In the other patients, the omentum was absent or too short to be interposed. Low and very-low anastomoses were performed using the same 31-mm diameter transanal end-to-end double stapling anastomotic device (DST series EEA [end-to-end anastomosis] 31 mm with 4.8-mm staples; Autosuture, Tyco, UK).
Sigmoid side-to-end and ileocecal latero–lateral anastomoses were manual 35-mm diameter anastomoses performed with Vicryl 3/0 (Ethicon, Neuilly-sur-Seine, France).
All surgical procedures were performed by the same gynecologist (V.A.) and the same digestive surgeons (A.B. and I. EN.), all of whom are skilled in surgical management of endometriosis and colorectal surgery.
Evaluation of postanastomotic strictures
AS is defined as the presence of different signs of constipation and the impossibility to pass through the anastomosis with a 12-mm diameter endoscope.14,15
Patients were asked about symptoms of constipation, abdominal bloating, and small-caliber stools preoperatively and postoperatively at 4, 8, 12, and 24 months after surgery. Patients were regularly seen at follow-up consultations. Patients presenting with these symptoms were suspected of having AS (Fig. 3).

Anastomotic stricture occurring 8 weeks after surgery. Left and right arrows show the presence of a severe anastomotic stricture.
Constipation is a symptom, not a disease. There is constipation if a patient presents with at least two of the following criteria (the ROME criteria)
16
:
• Fewer than three bowel movements (BMs) per week • Hard stool in more than 25% of BMs • A sense of incomplete evacuation in more than 25% of BMs • Excessive straining in more than 25% of BMs • A need for digital manipulation to facilitate evacuation.
A change in stool caliber is defined as the presence of some change in stool characteristics that allow it to be narrower. Usually, this is because the stools are softer. They can be molded by a lesion that narrows the diameter of the lumen or can result from colonic or anal disease.
Abdominal bloating is defined as a condition in which the abdomen feels full and tight. A patient's abdomen may look swollen (distended).14,15,17
Questionnaires were standardized and focused on symptoms of AS (see Table 2).14,15,17,18
Respondents were instructed: Choose “Yes” or “No” for each question, please.
Constipation
Question 1: “Do you have difficult passage of stools for several weeks or longer?” (yes/no?). Question 2: “Do you have infrequent bowel movements?” (yes/no?). Question 3: “Do you have less than three bowel movements a week?” (yes/no?).
Change in stool caliber
Question 1: “Did you observe a change in the caliber of stools over the time, so that they are thinner than before?” (yes/no?) yes/no?
Abdominal bloating
Question 1: “Do you feel that your abdomen feels more often full and tight or more swollen (distended) than before?” (yes/no?)
Predilatation setup
Patients suspected of having AS because of their responses to questioning underwent double-contrast barium enemas and the strictures were measured via barium enema on strict profile and anteroposterior positions (Fig 3).
A rectosigmoidoscopy was performed if the smallest diameter noted on a barium enema was <12 mm (Table 1; Fig. 3).
Anastomotic endoscopic dilatation
All patients with suspected AS, based on responses to questions and results of double-contrast barium enemas, were scheduled in the One Day Clinic both for diagnostic and therapeutic rectosigmoidoscopy under deep sedation (using propofol without endotracheal intubation). In the absence of signs of bowel obstruction, the usual bowel preparation was used (4 L of polyethylene glycol). Therapeutic endoscopes (GIF-1T 160 or CFQ-160; Olympus, Tokyo, Japan) enabled use of “through the scope” wire-guided balloon dilators of different diameters (from 10 to 20 mm, CRE, Boston Scientific, Natick, MA). This kind of device enables progressive dilatation (10–12, 12–15, 15–18 and 18–20 mm).
Endoscopic dilatation was chosen when the estimated residual lumen at the level of the anastomosis was <12 mm. The first target diameter was left to the clinician in charge of the patient according to the initial endoscopic appearance, as well as the need to perform a second dilatation. Dilatations were performed under endoscopic control, only 1 patient required a stent placement with fluoroscopic control.
Histology
Classical (hematoxylin and eosin) histology and CD-10 immunohistochemistry were performed in all resection specimens. CD-10 is the most reliable marker for endometriotic stromal cells. 19
CD-10 (neprilysin) immunohistochemistry was used to rule out metastatic cellular mesenchymal tumors of the uterus, 20 metastases of very well-differentiated gastric carcinomas of the intestinal type, 21 adenocarcinomas of the colon, 22 clear-cell urothelial carcinomas of the urinary bladder, 23 and metastases of thyroid carcinoma to the colon, 24 which are all CD-10–negative conditions.
Statistical analysis
Mean operating time, age, body mass index (BMI), follow-up, length of large-bowel resection, largest diameter of endometriotic nodules on the colon were compared between the group with confirmed symptomatic AS and the group without AS or without suspicion of AS (Table 3).
Results are expressed as means ± standard deviation.
p < 0.05 was considered to be significant with a two-tailed Student's t-test.
AS, anastomotic stricture; BMS, body mass index.
Statistical analysis was performed using a two-tailed Student's t test. A p-value of <0.05 was considered to be significant.
Results
Large-bowel resections and anastomosis
Results are expressed as means ± standard deviation (SD).
The mean operating time was 250 ± 64 minutes. The mean follow-up time was 64 ± 44 months.
A total number of 20 complications (18%) occurred in this consecutive series. Complications were divided into two groups: minor and major complications. Major complications were: anastomotic leaks (n = 3) and rectovaginal fistulae (n = 2).
Rectovaginal fistulae and anastomotic leaks occurred in patients who underwent posterior colpectomy. The mean diameter of stricture of patients who had anastomotic leaks was 14 ± 1.4 mm.
Minor complications (Table 1) were AS (n = 13) and voiding difficulties (n = 2).
The omentum was interposed between the rectal and the vaginal sutures in 8 (62%) of 13 cases of AS.
Pathology
Results are expressed as means ± SD.
Histology showed the presence of DIE in all resection specimens (N = 113), confirmed by CD-10 immunohistochemistry. Mean length of the large-bowel resection specimens was 14 ± 7 cm. The mean largest diameter of the colonic endometriotic lesions was 3.45 ± 2.4 cm.
Resection margins were free of endometriosis in all patients with AS.
Characteristics of AS
A total number of 25 patients were suspected of having AS based on questioning and underwent double-contrast barium enemas (Fig. 3). Thirteen patients (52%) had severe narrowing of the anastomosis (smallest diameter <12 mm seen on barium enemas) and underwent balloon dilatations. In those cases, it was impossible to pass through the stricture with a 12-mm diameter endoscope.
Those 13 patients did not present with symptoms of constipation preoperatively. All AS occurred after low or very-low resections associated with partial colpectomy and mechanical end-to-end colorectal anastomosis using a 31-mm diameter stapling device. No cases of AS occurred neither in the group of major complications nor in the group of segmental sigmoid resections (n = 27; Table1). The mean diameter of the stricture was 8.6 ± 1.1 mm, and the final diameter after dilatation was 14.3 ± 3.1 mm.
The mean distance between AS and the anal verge was 8 ± 2 cm. The mean delay of occurrence was 7.8 ± 1.2 weeks.
Eight patients (62%) had 1 dilatation. Five patients (38%) underwent a second dilatation and, among them, 4 (31%) had a third dilatation.
The total number of dilatations was 22 (Table 1).
The other 12 patients (48%) who had negative barium-enema results, but were suspected of having AS based on responses to questions (Table 2) underwent medical treatment until the patients were symptom-free.
Medical treatment consisted of increased liquid intake, high-fiber diet, and laxatives (paraffin oil) in case of failure. Patients were symptom-free after a period of 12 ± 2.4 weeks.
Anastomotic dilatation
Comparisons between mean operating time, age, BMI, follow-up time, length of large-bowel resection, largest diameter of the endometriotic nodule in the group with confirmed symptomatic AS and the group without AS or without suspicion of AS showed no statistical difference (Table 3).
The final mean diameter after dilatation was 14.3 ± 3.1 mm.
One patient had sepsis following dilatation and underwent a Gastrografin® enema showing the presence of a colonic intraparietal disruption. Before dilatation, the largest diameter of the stricture was 9 mm, and she had two dilatations. A resection of the anastomosis and a colonic J-pouch coloanal anastomosis with ileal protection for 6 weeks were necessary to correct the colonic fistula.
Discussion
Large-bowel resections for colonic DIE improves patients' quality of life but can be responsible for severe10–12 and functional complications.6,8–12 There are scanty data in the literature concerning AS after large bowel surgery for DIE.
The incidence of symptomatic AS in the literature ranges from 2% to 5%,14,25,26 but published series mostly concern colorectal carcinoma, Crohn's disease, and diverticulitis (based on a systematic search using MEDLINE,® EMBASE, Cochrane, and Web-of-Science Libraries).
In this series of 113 colonic resections, there was a much higher rate of AS corresponding to 12% of all colonic resections, which is more than was expected for other indications than endometriosis. These patients had no symptoms of constipation as noted during preoperative questioning and represent de novo AS cases. No stricture was observed after high resections (segmental sigmoid or ileocecal resections), which were manual anastomoses. However, studies comparing manual to mechanical anastomoses have been inconclusive.27,28 A recent meta-analysis failed to demonstrate any superiority of stapled over manual techniques for colorectal anastomosis, regardless of the level of anastomosis. 29
In the current study, all strictures occurred after low and very-low resections associated with partial posterior colpectomy, suggesting that the apposition of a digestive suture against a vaginal suture in an inflammatory area could be a key factor in the occurrence of AS. Eight patients with AS (62%) underwent interposition of the omentum between both sutures. This procedure is known to prevent fistulas, but its role in AS is not well-known. 30 The true etiology of AS is rarely known and could be multifactorial. An insufficient diameter of the anastomosis could theoretically be responsible for AS; however, a large diameter of 31 mm was used systematically.
The current authors cannot exclude the possibility that some ischemia occurred after mesorectal dissection, but neither signs of perianastomotic ischemia nor necrosis were found at rectosigmoidoscopy. The presence of a local, chronic allergic reaction of the colon wall to the staples could also be responsible for further strictures. In opposition with colorectal adenocarcinoma, which is primarily a mucosal disease, large-bowel endometriosis starts at the serosal aspect of the colon and the colonic mucosa is involved in ∼5% of cases. 31 Endometriosis is an inflammatory disease with peritoneal fluid containing high levels of inflammatory cells (macrophages, lymphocytes, plasmocytes, etc.). 32 Such an inflammatory microenvironment around the anastomosis could increase the possibility of further strictures. Finally, the presence of positive margins and residual disease on the anastomotic site could be another possibility, but margin sections in the AS group did not show any residual disease.
Several endoscopic dilatation techniques can be used and can be associated 33 with mechanical dilatations with the help of Savary probes or Eder olives, pneumatic dilatations with a balloon inserted in the stricture, pneumatic dilatations electroincisions, or the YAG laser and stenotomy (radial incisions in the anastomotic ring).
Pneumatic dilatations are generally preferred to mechanical ones because of a lower risk of mucosal laceration and perforation. Balloon dilatations are generally well-tolerated and 90% of patients are symptom-free after dilatation, but 2–4 procedures are often necessary to treat the stricture.33–35 In the 13 patients with confirmed AS, 22 dilatations under general anesthesia were necessary to correct the strictures, with some patients requiring 3 procedures (Table 1). A 2%–3% rate of complications is generally associated with pneumatic dilatations. Some of them (small amount of bleeding, mucosal lacerations) generally heal spontaneously. More severe complications (perforation, disruption of the large bowel, leaks) often require surgery, resection of the suture, refection of the anastomosis, and, eventually, protective derivation. 36 In cases of failure of dilatations with persistence of long and fibrous stenosis, surgery or placement of a metal stent are common alternatives.36–38 However, metal stents are generally reserved for patients with colonic carcinoma who are in subocclusion before elective surgery or as palliative treatment for patients with inoperable conditions. 38
One of the limitations of the current study is that the incidence of AS in asymptomatic patients was unknown. In order to avoid that drawback, rectosigmoidoscopy had to be performed postoperatively in all patients. Also it must be highlighted that AS symptoms can diminish or even disappear with time when a patient is receiving medical therapy, but spontaneous healing rarely occurs when the stricture is <12 mm diameter.16–18 Interestingly, 3 patients who had very-low resections developed AS, which could be attributed to the type of anastomosis (mechanical end-to-end anastomosis). In those cases, transverse coloplasty or the confection of a colonic J-pouch–anal anastomosis are probably more appropriate.39–42
Conclusions
In this series, AS was a frequent complication after colorectal resection and anastomosis for DIE of the large bowel. AS can be responsible for severe discomfort and may require several dilatations under general anesthesia. AS occurred after low and very-low resections associated with partial posterior colpectomy, even with omental interposition. Surgeons dealing with DIE of the colon should be aware of this complication and inform patients clearly about this potential functional complication. Further comparative studies based on this specific complication are necessary before drawing definitive conclusions about prevention and the most adequate treatments.
Footnotes
Disclosure Statement
No competing financial conflicts exist.