
Abstract
Abstract
Introduction
T
Case
A 70-year-old female, gravida 1, para 1, presented through referral for management of large uterine leiomyomata. The patient complained of abdominal and lower-back pain along with increasing abdominal girth. She denied any episodes of postmenopausal bleeding. Pertinent facts in her history also included many comorbidities and a history of a nephrectomy.
A pelvic computed tomography (CT) scan performed 4 months prior to her visit was remarkable for 2 uterine leiomyomata that measured 8 cm on the right and 7 cm on the left. A repeat pelvic CT scan performed 3 months later was suspicious for uterine leiomyomata, but could not be used to rule out leiomyosarcoma (Fig 1). The uterine leiomyomata now measured 10 cm and 7 cm, respectively. A 7-cm hernia in the left lumbar triangle with large-bowel herniating was also noted. Follow-up magnetic resonance imaging was performed 21 days later and was remarkable for an enlarged uterus with 2 masses suggestive of leiomyomata. The right mass measured 8.6 cm, and the left mass measured 11.5 cm.

The arrow is pointing to endometrial stromal sarcoma.
Following appropriate consultation, it was recommended that the patient undergo a hysterectomy for suspected benign disease. An attempt at an endometrial biopsy was unsuccessful secondary to severe vaginal atrophy and patient discomfort. She was referred to the general surgery department for evaluation of a 7-cm lumbar triangle hernia in the setting of abdominal and back pain. Secondary to many comorbidities, she was referred for medical clearance. Finally, she was scheduled to undergo total abdominal hysterectomy and bilateral salpingo-ophorectomy.
On the day of surgery, while waiting in preoperative holding, the patient was noted to be ill-appearing and was complaining of severe abdominal pain, shortness of breath, and fatigue. Laboratory tests were performed and found to be remarkable for significant hyperglycemia and elevated serum creatine kinase MB. Hemoglobin was stable, and the remainder of her cardiac workup showed benign results. This patient became tachypnic with decreased O2 saturation. Her past medical history was negative for diabetes; nonetheless, with her presentation, diabetic ketoacidosis was highly suspected. The decision was made to postpone surgery until the patient could be stabilized.
The patient was transferred to the emergency room for further evaluation and treatment. Secondary to extreme abdominal discomfort, a repeat CT of the pelvis was performed and found to be remarkable for hemoperitoneum with a sentinel clot located on the right 8.6 cm leiomyoma, suggesting it to be the origin of the intra-abdominal hemorrhage (Figs 2 and 3). This new finding increased the suspicion of a uterine sarcoma further.

The arrow is pointing to hemoperitoneum.

The arrow is pointing to a sentinel clot.
The gynecology–oncology service was consulted. An emergent total abdominal hysterectomy and a unilateral salpingo-ophorectomy with staging were performed. Approximately 2 L of blood were removed intraoperatively and confirmed to have originated from an 18.5 × 12.8 × 10.5–cm mass that was suspicious for leiomyosarcoma on frozen section. The mass was intramural, soft, and fleshy, with patchy areas of hemorrhage located on the fundal portion of the uterus. There was extensive hemorrhage on the posterior aspect of the tumor. The tumor invaded >50% of the myometrium. The cervix, fallopian tubes, ovary, and omentum were not involved. Mitotic activity was variable throughout the tumor, ranging from 5 to 9 mitoses per 10 high-power fields with rare foci showing up to 12 mitoses per 10 high-power fields (Figs. 4 and 5). Extensive tumor invasion of vascular channels were noted (Fig. 6). The tumor was strongly and diffusely immunoreactive for estrogen receptors (ERs) and progesterone receptors (PRs). Total uterine weight, including the mass, right ovary, and fallopian tube was 1646 g. Final pathology was remarkable for low-grade ESS stage 1b NX ER+/PR+ (Fig. 7).
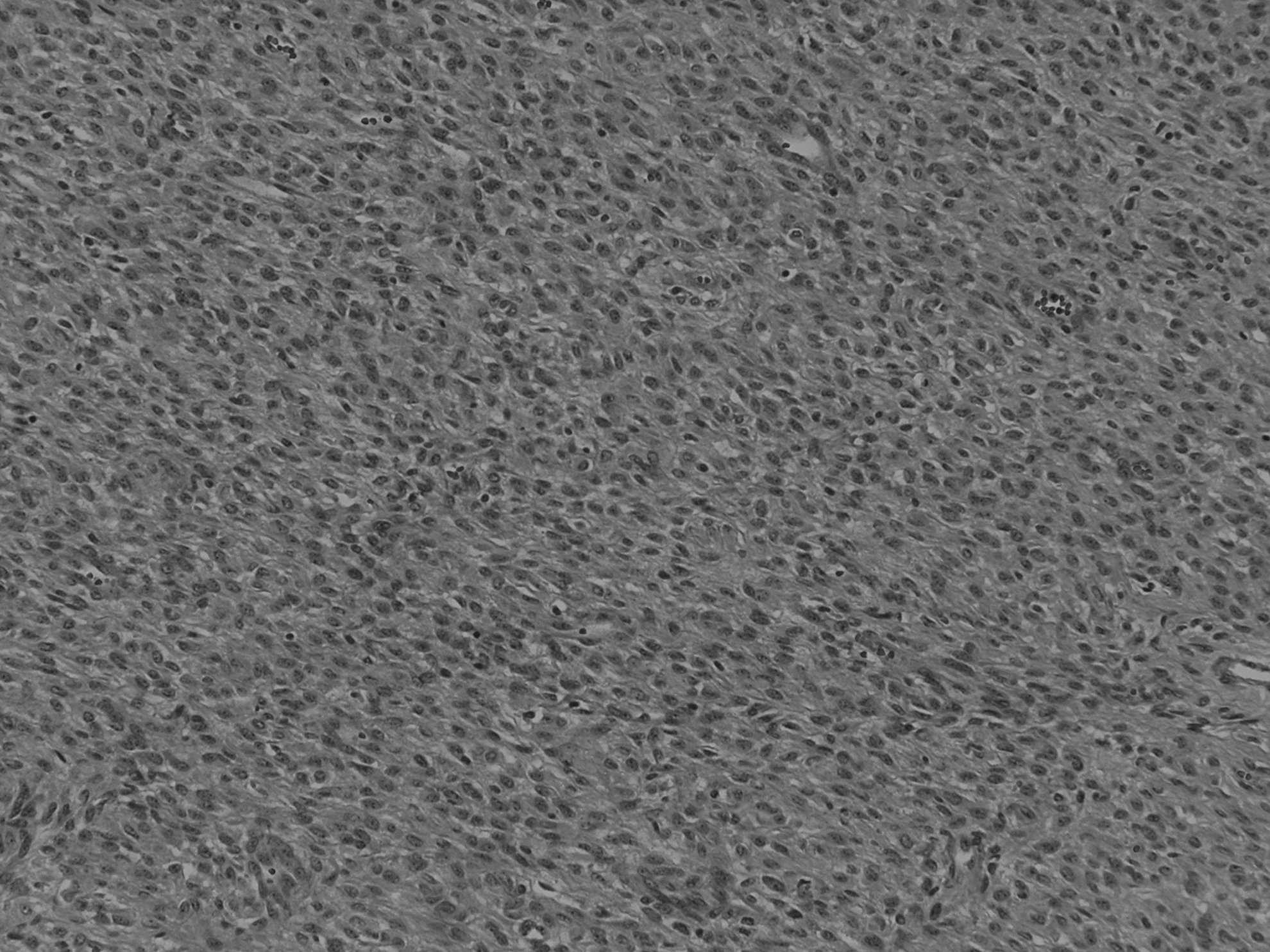
(H&E, 100×) The tumor consisted of diffuse sheets of round to oval cells with poorly defined cell borders in a vascular stroma.

(H&E, 400×) Tumor cells had mild nuclear atypia, delicate chromatin, and inconspicuous nucleoli. Mitotic figures were identified.
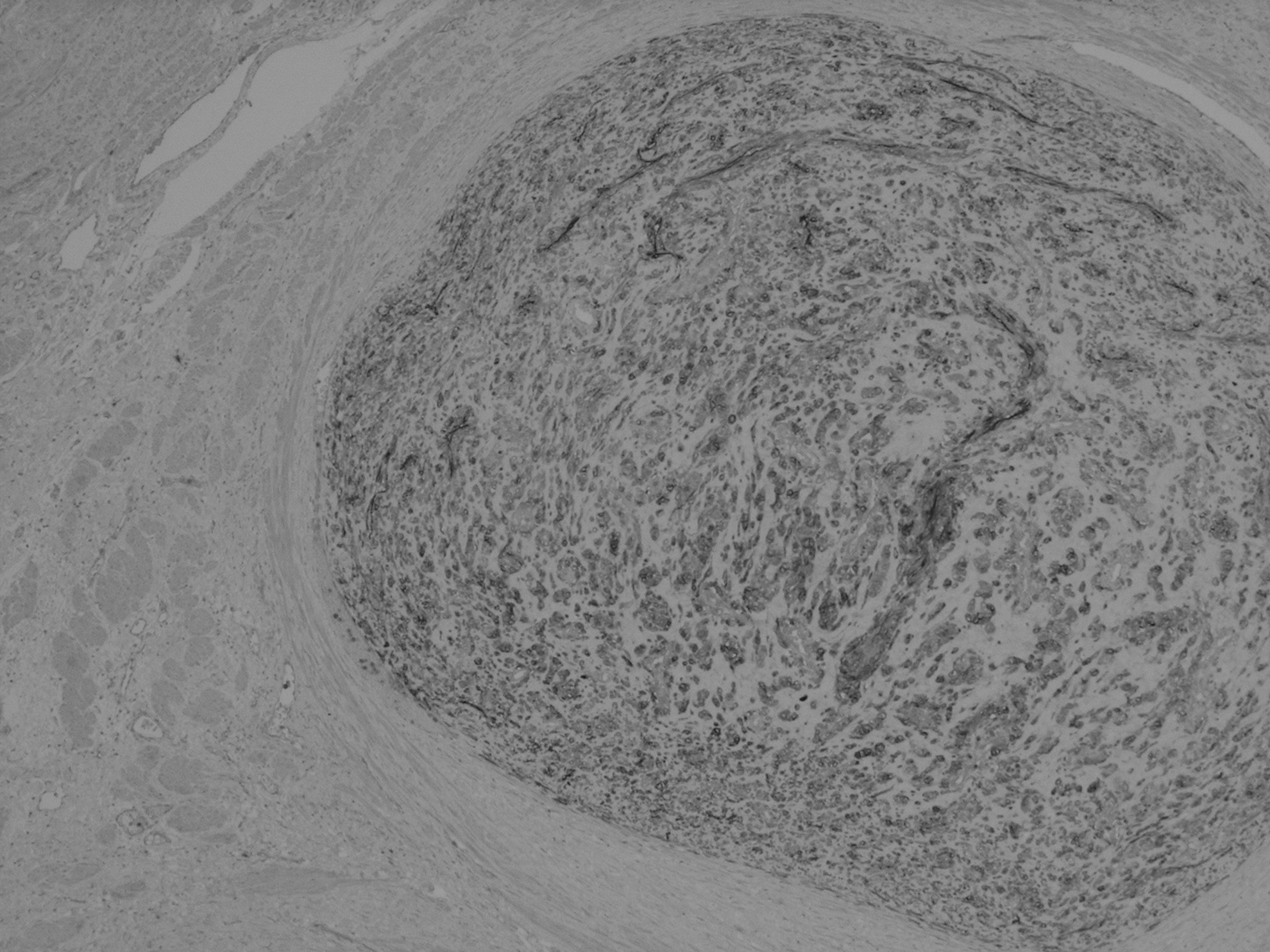
(CD10, 40×) CD10 immunoreactive tumor was seen within vascular spaces.
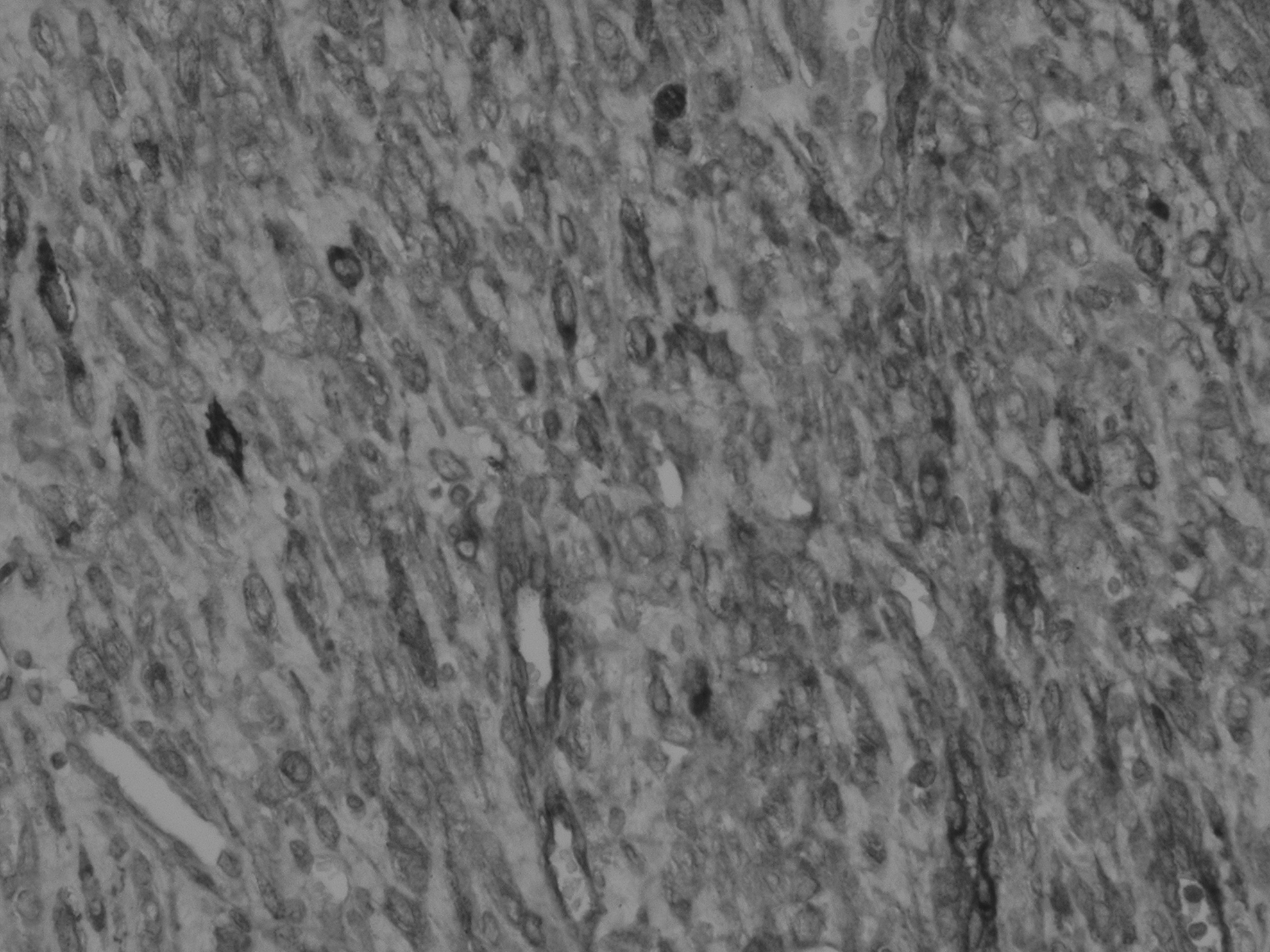
(CD10, 200×) Tumor cells were positive for CD10, thus supporting the diagnosis of endometrial stromal sarcoma.
Results
On postoperative day (POD) #1 this patient was started on carboplatin and paclitaxel. She was extubated successfully on POD #3 and discharged to home on POD #6. Megestrol was prescribed and eventually changed to anastrozole secondary to undesired side-effects. The patient remained stable in the outpatient setting, and she is continuing care within the gynecology–oncology service.
Discussion
A review of the literature using PubMed and the terms
Sarcomas are typically diagnosed between ages 50 and 60. The majority of sarcomas are diagnosed after hysterectomy; however, carcinosarcoma may often be diagnosed at the time of endometrial biopsy. 1 In the current patient, an endometrial biopsy was unsuccessful. Pathology revealed ESS with predominantly myometrial growth; therefore, an endometrial biopsy would have likely not been diagnostic.
Uterine sarcomas metastasize early secondary to hematogenous spread, primarily to the lungs. In the current case, the patient's pathology was remarkable for extensive vascular invasion. A chest X-ray was not suggestive of metastasis. Para-aortal lymph-node dissection was not recommended given that lymph-node metastasis is seen in <3% of cases. 5 Rupture of uterine sarcomas are thought to occur secondary to degeneration and tumor necrosis. Hemorrhage may be caused by the rupture of superficial and deep blood vessels secondary to erosion of the vessel walls. 6
ESS is classified further into two subgroups: (1) low-grade ESS and (2) undifferentiated endometrial sarcoma. Treatment is often based on operative debulking and chemotherapy. 7 Low-grade ESS, which tends to be hormone-sensitive, as reported in the current patient, has an overall 5-year survival rate of 73%–100%. Undifferentiated endometrial sarcoma, formerly known as high-grade ESS, has a much lower 5-year survival rate of 25%–55%. 3
Conclusions
This report highlights the rare manifestation of the only reported low-grade ESS rupture resulting in spontaneous hemoperitoneum in a patient with suspected uterine leiomyomata. The majority of the literature reported on uterine sarcomas, focusing on leiomysosarcomas. Endometrial biopsies often are not helpful in diagnosis. Diagnosis is often delayed. Prognosis of ESS is more favorable than leiomyosarcoma; however, in the setting of tumor rupture, ESS can be equally fatal. Recurrence rates tend to be high secondary to early hematogenous spread. In the setting of uterine leiomyomata associated with spontaneous hemoperitoneum, ESS should also be included in the differential diagnosis.
Footnotes
Author Disclosure Statement
No competing financial conflicts exist.