
Abstract
Abstract
Introduction
F
There are several treatment options for fallopian-tube prolapse. In this case, a laparoscopic approach was chosen.
Case
The local ethics committee approved this case report and informed consent was obtained from the patient. She was a 45-year-old woman, gravida 2, para 2, who was admitted to the clinic at Gulhane Milidary Medical Academy, in Etlik, Ankara, Turkey, because of postcoital vaginal bleeding and pelvic pain for a duration of 1 year. She had a previous total abdominal hysterectomy, with conservation of the fallopian tubes and ovaries, 13 months prior at a different hospital because of abnormal uterine bleeding. Thus, patient's abdominal hysterectomy operation records were unavailable, so it was not known if the patient's parietal peritoneum was closed at the time of that surgery.
A gynecologic examination revealed a 3-cm diameter, polypoid reddish mass protruding from the vault into the vagina (Fig. 1A). The mass was deemed to be a fallopian tube because of its fimbrial gross appearance. An ultrasonographic examination revealed a 3-cm left ovarian endometrioma.
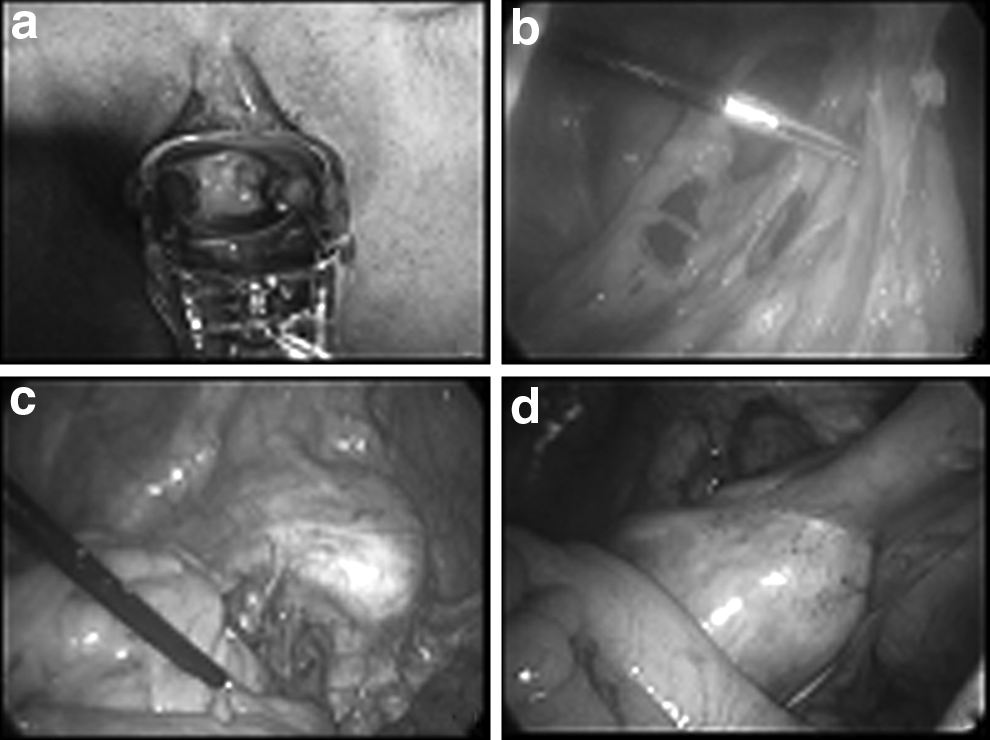
Fallopian-tube prolapse into the vault. Dense adhesions among the anterior abdominal wall
A laparoscopic exploration showed dense adhesions among the anterior abdominal wall, omentum, and bowels that obliterated the cul-de-sac. Dense adhesions were also noted between the bowels and left fallopian tube, which protruded into the vaginal vault and left ovary (Fig. 1, B, C, & D). A Breisky-Navratil retractor was used vaginally to elevate the vault to facilitate adhesiolysis and surgery. The adhesiolysis was performed with a harmonic scalpel. The left ovary was dissected from the bowels and fallopian tube, and a left salpingo-oophorectomy was performed. The protruding fallopian tube was dissected from the vault, and the tube was pulled up to the abdomen with a clinch (Fig. 2, A & B). Prophylactic right salpingectomy was also performed. A 2-cm peritoneal vaginal fistula was closed with No. 2/0-coated Vicryl® polyglactin 910 (Ethicon) by intracorporeal suturing (Fig. 2, C & D). The operation time was 80 minutes, and her estimated blood loss was 100 cc.

Results
This patient was discharged uneventfully on the first postoperative day. At a follow-up examination 3 months later, she was completely well.
Discussion
There are several treatment options for fallopian-tube prolapse into the vaginal vault. Historically, fallopian-tube prolapse was treated vaginally with a silver nitrate application. 2 However, this is not a recommended treatment modality because of its unsuccessful results and the risk of iatrogenic scarring and vaginal stenosis.2,8 Immediate partial resection of a prolapsed fallopian tube by a vaginal or abdominal route is possible, but this requires a second repair surgery. 8
The goal of fallopian-tube prolapse treatment is to remove the fallopian tube totally from the vault and close the peritoneal vaginal fistula. Total salpingectomy is necessary for treating the patient sufficiently.3–5,9 Total salpingectomy by vaginal, abdominal, or laparoscopic approaches, or a combination of these techniques have been described as treatment options.8,10,11 Surgical experience, equipment, and the patient's clinical status are important factors to consider when selecting the type of surgery. 8 However, surgery via the vaginal route is not suitable for patients with dense adhesiolysis in the pelvis because of limited visualization of pelvic adhesions.
The current patient was treated with total salpingectomy via a laparoscopic approach instead of laparotomy or a vaginal route. The current authors believe that laparoscopic access has several advantages, such as visualization of the pelvis and ease of adhesiolysis with modern equipment, including a harmonic scalpel (Ethicon), LigaSure (Covidien,
Maintaining meticulous hemostasis and preventing vault infection can combat fallopian-tube prolapse.2–4 Correct surgical techniques and closing the parietal peritoneum are also important.2–4 In addition, prophylactic bilateral salpingectomy can be performed to prevent fallopian-tube prolapse or to prevent fallopian-tube or ovarian cancer.12–17
Conclusions
Surgeons should keep in mind the possibility of fallopian-tube prolapse when the fallopian tubes and ovaries are conserved after a hysterectomy. Laparoscopic access is a feasible method for successfully treating fallopian-tube prolapse, secondary to a hysterectomy.9,18 Using the Breisky-Navratil retractor to elevate the vault makes it easier to perform pelvic adhesiolysis.
Footnotes
Author Disclosure Statement
The authors declare that there are no conflicts of interest.