
Abstract
Abstract
Introduction
D
A rudimentary horn might or might not have functional endometrium, might or might not be communicating with the unicornuate uterus, and might be attached to the surrounding organs by only a fibrous band. Magnetic resonance imaging (MRI) remains the gold standard for diagnosis of these uterine anomalies. 2
The incidence of uterine anomalies in the general population is estimated at 0.5%, with unicornuate uterus accounting for ∼5% of these anomalies. 3 While the majority of these anomalies are asymptomatic, they may result in gynecologic problems, including primary amenorrhea, pelvic pain, and endometriosis secondary to retrograde menstruation. Uterine anomalies are also known to be associated with higher adverse pregnancy outcomes with decreases in live birth rates, as well as increased risks of malpresentation, growth restriction, prematurity, intrauterine fetal demise (IUFD), miscarriage, and ectopic pregnancy. 3
Because of the risk of ectopic pregnancy, excision of a rudimentary horn has been recommended prior to conceiving. Both open and laparoscopic techniques have been described previously.4,5
The following is a case report of an ectopic pregnancy in a noncommunicating rudimentary horn in a woman who underwent subsequent robotic-assisted resection. This case was deemed exempt from institutional review board approval by the Hawaii Pacific Health Research Institute.
Case
The patient was a 29-year-old, gravida 1 female at 9 weeks' gestational age, who presented with a positive pregnancy test. She was asymptomatic with normal vital signs. Her examination was benign, and a review of her systems was negative for abdominal pain or vaginal bleeding.
Pelvic ultrasound was performed, which revealed an embryo measuring 8 weeks and 0 days by crown-rump length with cardiac activity located in the uterine cavity on the left side. The left cavity appeared to be separate from the right uterine cavity, with the cervix connected to the right uterine horn. An MRI was obtained, which revealed fluid collection consistent with gestation in the left uterine horn surrounded by very thin myometrium. No communication was visualized between the right and left endometrial cavities. A 2-cm myometrial stalk was seen connecting the left uterine horn to the lower uterine segment/upper cervical region of the dominant right horn.
A recommendation was made at this time to proceed with surgical intervention for an ectopic pregnancy in the noncommunicating rudimentary uterine horn. Because of the robotic surgical expertise in the gynecologic oncology department, she was referred there for robotic-assisted excision.
This patient was taken to the operating room for a robotic resection of the left uterine horn and the intrauterine pregnancy, and a left salpingectomy (Intuitive, Sunnyvale CA). Intraoperative findings were significant for a left uterine horn with a pregnancy, which appeared to be ∼10 weeks' size with extraordinary vascularity. An attachment was seen between the left and right horns; it was ∼3–4 cm in length and 0.5 cm in thickness (Fig 1). The left retroperitoneal space was opened and the ureter was identified. The uterine artery feeding the uterine horn was identified, cauterized, and divided. The left fallopian tube was separated from the ovary, which retained its vascular supply. The left uterine horn was detached from the lateral surrounding attachments. Medially, a thick fibrous attachment with no lumen was divided between the uterus and horn. The uterine horn and fallopian tube were placed in a bag, opened to confirm pregnancy, morcellated, and removed from the abdomen through a 10-mm port. Hemostasis was obtained with coagulation. The procedure was uncomplicated, with an estimated blood loss <25 mL.
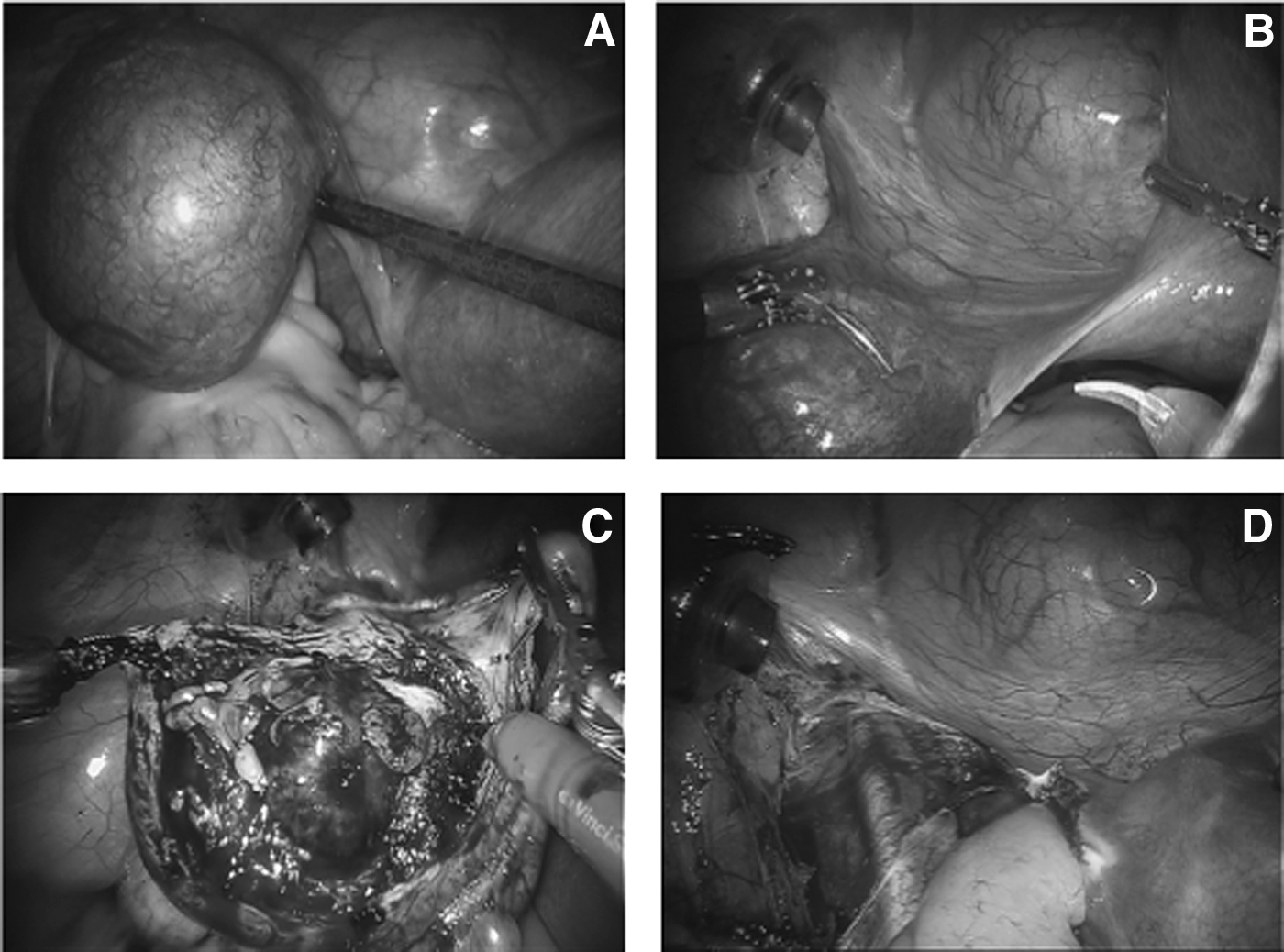
Intraoperative findings.
Results
There were no postoperative complications. The patient's pathology was consistent with a tubal/cornual ectopic pregnancy. She stated that she would like to conceive in the future. Any future pregnancies in this patient will need to be monitored closely because of her risk of a higher complication rate. 3
Discussion
The patient described above was diagnosed with a unicornuate uterus with a noncommunicating rudimentary horn as visualized on MRI and pelvic ultrasound. As described previously, pregnancies in women with uterine anomalies are at increased risk of poor outcomes such as malpresentation, preterm delivery, lower birth rates, and IUFD. Reichman et al. 3 included a review of 290 women with unicornuate uteri, of which 175 conceived, with a total of 468 pregnancies. In this review, the researchers noted a live birth rate of 49.9%, with only 44% occurring at term. The preterm delivery rate was 20.1%. There were increased rates of first-trimester abortion (24.3%) and second-trimester abortion (9.7%). There was also an increased rate of IUFD at 10.5%. The ectopic pregnancy rate observed in this population was 2.7%.
The risk of rupture of an ectopic pregnancy is ∼80% by the second trimester, likely because of the thin surrounding myometrial mass. 1 Multiple case reports have described complications associated with pregnancy in a non-communicating rudimentary uterine horn.6–10
Recommended treatment is complete removal of the rudimentary horn and fallopian tube on the affected side. The ideal time for removal is prior to conceiving; however, this may be a challenge because of the difficulty in diagnosis. Many of these anomalies are asymptomatic, they might not be obvious on physical examinations, and the imaging modalities for diagnosis are invasive.
Both open and laparoscopic techniques have been utilized in the removal of a rudimentary horn in the past. This is the first reported case describing a robotic-assisted removal. In this case, the surgeon elected to proceed with a robotic-assisted resection to better isolate and identify the blood supply and other nearby pelvic structures. Previous cases of uterine-horn ectopic pregnancies have resulted in significant blood loss; therefore, the robotic approach was considered ideal, as precise control of anomalous vessels would result in significantly less blood loss. Over the past 10 years robotic surgery has become more common in gynecology practice. Advantages include visualization, surgical precision, and decreasing fatigue and tension tremors. 11 A recent case report described the use of robotic surgery in the excision of a cesarean-scar ectopic pregnancy and hysterotomy revision, 12 an example of the growing utility of the robotic approach.
Thus far, studies comparing benefits of robotics over laparoscopy for gynecologic surgery have been inconclusive. Previous studies have focused on increased cost of the procedure without statistically improving the rate of complications. However, some trials have noted a decrease in hospital stay.13,14 This has remained a controversial topic largely due to the limited number of randomized controlled trials as well as bias involved in observational studies. The decision to proceed with robotic surgery over laparoscopy in this case was made based on the complexity of the case as well as provider expertise and comfort with the surgical approach.
Conclusions
In the past, the patient in this case would likely have undergone an open procedure at risk for high blood loss and a prolonged recovery time. With the use of this approach, the patient underwent an uncomplicated, minimally invasive procedure with minimal blood loss. This report represents the first reported case of robotic removal of a rudimentary horn ectopic pregnancy.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.