
Abstract
Abstract
Introduction
A
The signs following major vascular laceration are: abrupt drop in blood pressure (BP); tachycardia; decrease in end tidal CO2. Intraperitoneal bleeding might or might not be evident; however, retroperitoneal hematoma will always be noted if the surgeon looks for it. A steep Trendelenburg position may initially mask such findings, but blood volume will diminish and the blood will accumulate retroperitoneally.
This article is a sequel to an earlier report of 31 major vessel injuries published in this journal in 2003. 1 In addition, this newer article is an extension of prior reports dealing with force required to thrust the primary trocar through the anterior abdominal wall, 2 and in vivo, prospective measurements of the aorta and iliac vessels in reference to their distances from the anterior abdominal wall, with patients undergoing modified lithotomy as well as being in the Trendelenburg position during actual laparoscopic surgery. 3
This current study focused on information that will, it is hoped, result in rapid diagnosis and prompt life-saving treatment of this type of injury. Furthermore, the author hopes the included data will enable gynecologic surgeons to avoid creating such injuries in the first place. Major vessel injury is, in fact, an avoidable complication. Although a minority of major vessel intrusions occurs during the operative phase of the laparoscopic procedure, precise knowledge of pelvic anatomy and skilled, safe dissection techniques will likewise minimize this complication from occurring.
Materials and Methods
Records for women sustaining major vessel injury in conjunction with laparoscopic surgery were obtained between 1995 and 2015 (20 years). These cases emanated from medical–legal proceedings, hospital quality-assurance data, and cases shared by practicing physicians. The two time periods during which data was collected were 1995–2003 and 2004–2015. Using the collected data, the author was able to calculate body mass index (BMI), vessel(s) injured, management, collateral injuries, and outcomes.
In many instances, blood/blood-product replacement was not quantified accurately. Estimations of blood loss were also not accurate in most instances, because suctioned volume, which was recorded in anesthesia records irregularly, did not account for residual blood remaining in the abdomen, soaked pads, drapes, and clots. The actual loss was definitely underestimated in the majority of cases. Likewise time (minutes) elapsed until general surgeon or vascular surgeon arrival was charted irregularly by the circulating nurses or anesthesia teams. In general, the quality of recorded events postinjury was inferior relative to time intervals and specific remedial actions taken. These deficiencies held true for specifics relative to when correct diagnoses were made and when laparotomy was performed. When semi-reliable times were available as well as appropriate narratives, this information was added to the reportable data.
The cases were organized according to calculated BMI and designation or phase of the procedure (i.e., entry or operative). Finally, based principally on the time of the injury as well as the physical size of the injury, a designation was assigned to the offending instrument.
Results
A total of 68 vessel lacerations occurred among 64 patients. The vast majority of cases, 50/64, involved overweight or obese women (Table 1). All cases were subdivided according to the time-phase of the procedure when the injury happened (i.e., at entry or during the surgical operation). Table 2 illustrates that most of the injuries occurred during entry (54/64). Table 3 shows that 51/64 cases were related to trocar entry, whereas only 3 cases were thought to be created by Veress needle insertion. Ten cases were attributed to dissection techniques with or without energy devices. Table 4 identifies the 68 vascular injuries based on the vessel(s) lacerated at any phase of the laparoscopic procedure.
BMI, body mass index.
Concurrent laceration artery/vein: 4.
External iliac vessel, internal iliac vessel, and mesenteric vessel.
Clearly, the vessels injured most often were common iliac arteries and/or veins. The aorta or vena cava were lacerated 7% and 6% of the time and, together, accounted for 13% of the total vascular injuries. Nineteen of sixty-eight injuries were identified in external iliac, internal iliac, superior mesenteric, or inferior mesenteric vessels, or their branches or tributaries. In addition, several injuries occurred concurrently to more than one vessel (e.g., common iliac artery and vein, aorta and inferior vena cava). Some were via through-and-through penetration (i.e., piercing the anterior wall of the vessel and exiting the posterior wall). The latter type of injury created significantly greater damage and resulted in more blood loss as well as greater difficulty and more time to repair. Table 5 lists 20 deaths that were caused directly by vascular lacerations. Of these 20 mortalities, the greatest number were secondary to iliac artery and vein damage, with equal numbers of arterial versus venous lacerations. The mortality rate of 31% reflects the lethal reality of these injuries, compared to intestinal and urinary-tract complications.
Superior mesenteric and inferior mesenteric vessels.
The very first sign of major vessel injury, regardless of cause or location or—for that matter—body habitus, was within each anesthesia record. Sudden drop in BP, concurrent tachycardia, and sudden reduction in end tidal CO2 proved to be accurate predictors of what would evolve as catastrophic hemorrhage and a resultant fall in cardiac output.
Commonly, the anesthesia records demonstrated temporary measures, such as pressor drug administration, which only served to delay diagnosis and masked the actual cause of the sudden hypotension. Unfortunately, the same anesthesia records did not show any evidence of a differential diagnosis inclusive of major vessel injury to explain the recorded events. The gynecologic surgeons also failed to render early diagnosis unless they saw significant intraperitoneal bleeding. Retroperitoneal hematomas were not commonly investigated, not commonly identified, and not commonly connected with the recorded hypotension and tachycardia. The aforesaid was particularly the case when a patient was placed in a steep Trendelenburg position, as was frequently utilized during laparoscopic robotic surgery.
The mean blood loss following vascular laceration in this series was between 2500 and 3500 mL, which translates to a decrease in total blood volume of >50%. Initial replacement comprised large volumes of lactated Ringer's solution, followed by packed red cell transfusion and, finally, plasma. Platelet replacement and cryoprecipitate were administered late after coagulopathy had transpired.
Eleven patients lapsed into a pulseless electrocardiographic state before the correct diagnosis was made and appropriate action was initiated to control the hemorrhage.
Box 1 shows additional complications beyond the vascular damage. Coagulopathy was observed in all 20 cases in which the patients subsequently died as well as in 11 other cases in which the patients survived (i.e., a total of 31/64; 48%).
• Ureteral injury
• Lymphedema/thrombosis
• Inferior extremity amputation
• Neurologic injury
• Intestinal perforation
• Intestinal necrosis secondary to ischemia
• Compartment syndrome
• Suture of wrong vessel
• Systemic inflammatory response syndrome
• Coagulopathy
• Infection
• Respiratory failure
• Cardiomyopathy and heart failure
• Renal failure
Bowel injury concurrent with major vessel injury creates significant problems. In 2 cases, transverse-colon perforation occurred. These cases were associated with robotic laparoscopy where primary trocar entry was supraumbilical. The colonic injury was missed during the repair of the vascular laceration, which incorporated Dacron/Gortex interpositioned grafts between the distal aorta and the common iliac artery. Subsequently, the collateral bowel injury was diagnosed and a bowel resection was performed. Because of the probable contamination of the vessel graft, the vascular surgeon was obliged to remove the graft via another laparotomy and substitute a femoral vein autograft.
One case involved an anterior-wall injury to the external iliac artery. Primary repair with a 5-0–prolene suture was carried out by a general surgeon. The vessel's diameter was clearly reduced, but the surgeon felt that he could palpate a dorsalis pedis pulsation. During the night, the patient developed a cold leg, requiring an emergency laparotomy, iliac-segment resection, and interposition of a vascular graft. Twenty-four hours later, it was apparent that the graft had thrombosed and distal embolization had occurred, because the patient's leg was cold and blue, and lacked distal pulses. The patient subsequently underwent above-the-knee amputation.
Three cases of distal inferior-extremity compartment syndrome and 2 cases of abdominal compartment syndrome were observed. Fascia incision was required in the former and laparotomy with delayed wall closure was required in the latter. One patient who survived aortic injury and required five additional surgical procedures developed encephalopathy, which resulted in a permanent neurologic deficit. One patient who was diagnosed by the general surgeon-consult as having a vena cava laceration went into cardiac arrest during the repair operation but was revived. This patient was emergently transferred from the surgery center site to a neighboring hospital where she again arrested and could not be resuscitated. A postmortem examination revealed a vascular laceration of the right common iliac artery and vein but no injury to the vena cava. Death was attributed to exsanguination. Several sutures were described in an otherwise intact inferior vena cava but not one single stitch had been placed in the lacerated right iliac artery or vein.
Discussion
The injuries described herein are not only serious but are potentially lethal. When a major artery or vein is lacerated, a reflex emotional shock is instantaneously sustained by the operating surgeon and the anesthesia team. Given that these injuries are uncommon, no one is experienced in management other than military-trauma surgeons and military anesthesiologists who have dealt with battlefield wounds. The typical operating room (OR) reaction to massive, sudden hemorrhage is initially pandemonium. Correct treatment relies on prudent, timely accurate diagnosis and organization. Although a few case reports describe successful laparoscopic repairs,4,5 this type of decision is not wise. Immediate laparotomy via a generous midline incision is the most conservative and most appropriate procedure to be carried out.
Given that these injuries occur within the retroperitoneal space, precise knowledge of which vessel has been injured is not initially known. Gynecologists are not trained to repair great vessel lacerations. In order not to compound the damage, the best course of action for the gynecologic surgeon is to open the abdomen, apply manual pressure to the general area of the injury, and call for emergency general surgery or for vascular surgery intraoperative consultation.
The anesthesiology team should likewise call for immediate assistance. Multiple vessel access for the administration of blood and blood products must be obtained rapidly. One member of that team should be designated as the recorder, whose responsibilities include memorializing event times, patient response, fluid and blood-product volume administered, blood loss, laboratory reports, drugs administered including dosages, and personnel involved in the resuscitation. The same individual should liaison with the OR nursing staff. It is important to simultaneously inform the patient's family of the complication and the progress of the resuscitation. Tools such as cell savers must be immediately brought into the OR and put into service. Blood samples should be obtained for determining complete blood count, electrolytes, clotting factors, degradation products, calcium levels, and blood gases. All of the aforesaid needs to be accomplished systematically and simultaneously.
Avoiding major vessel laceration is infinitely better than having to manage such a catastrophe.6,7 Three variables relate to safe laparoscopic entry techniques: (1) angle of trocar/needle insertion; (2) depth control of the entry device; and (3) deviation from the midline relative to periumbilical thrust. During the laparoscopic operative phase, three variables likewise apply to safe surgical maneuvers: (1) expert knowledge of pelvic anatomy; (2) skillful dissection techniques, including safe use of energy devices; and (3) maintenance of a clear operative field of view.
The current study demonstrated repeatedly that, at the periumbilical location, major vessel injury could not anatomically occur unless a Veress needle or trocar was directed at or about an entry angle of 90°. Based on several published studies,8–10 these injuries will not happen without deep entry thrusting of a needle or trocar. Iliac injuries, with the exception of lacerations to the left common iliac vein, will not occur if entry is made in the midline (i.e., not deviated to right or left of the midline).
Narendran and Baggish 3 performed prospective measurements during actual laparoscopic procedures to determine distances between the anterior abdominal wall and the great vessels located in the posterior retroperitoneum in >100 women. Hurd et al. 11 performed similar measurements retrospectively, using computed tomography (CT) and magnetic resonance imaging (MRI) scans unrelated to actual laparoscopic procedures. Both studies demonstrated that the distances to the great vessels increased proportionately to the patient's BMI, with the greatest distances occurring in the obese category. The question not answered by either study was: “Why do obese women have the highest risk of major vessel injury?” In addition, the distance between the peritoneum of the anterior abdominal wall and the peritoneum covering the posterior retroperitoneal space before and during trocar thrust was not reported in the previously cited studies.
Quantification of the excursion distance of the anterior abdominal wall inward when a force is applied is a key factor needed to provide the answers to the question and issue posed above. A related piece of information relates to whether differences exist based on BMI between inward excursion of the anterior abdominal wall when a force is vectored toward the vertebral column. Reduced to its lowest common denominator, the problem hinges on abdominal-wall elasticity.
The author has observed that the abdominal walls of non-obese/thin women are less yielding to an applied force (i.e., a trampoline-like force; Fig. 1) In contrast, obese women's' fat-laden, thicker abdominal walls are lax and have significantly greater elasticity compared to non-obese patients' abdominal walls.
The abdominal wall of a non-overweight woman is shown. When a trocar force is applied, the relative rigidity of the anterior abdominal wall results in only limited inward excursion.
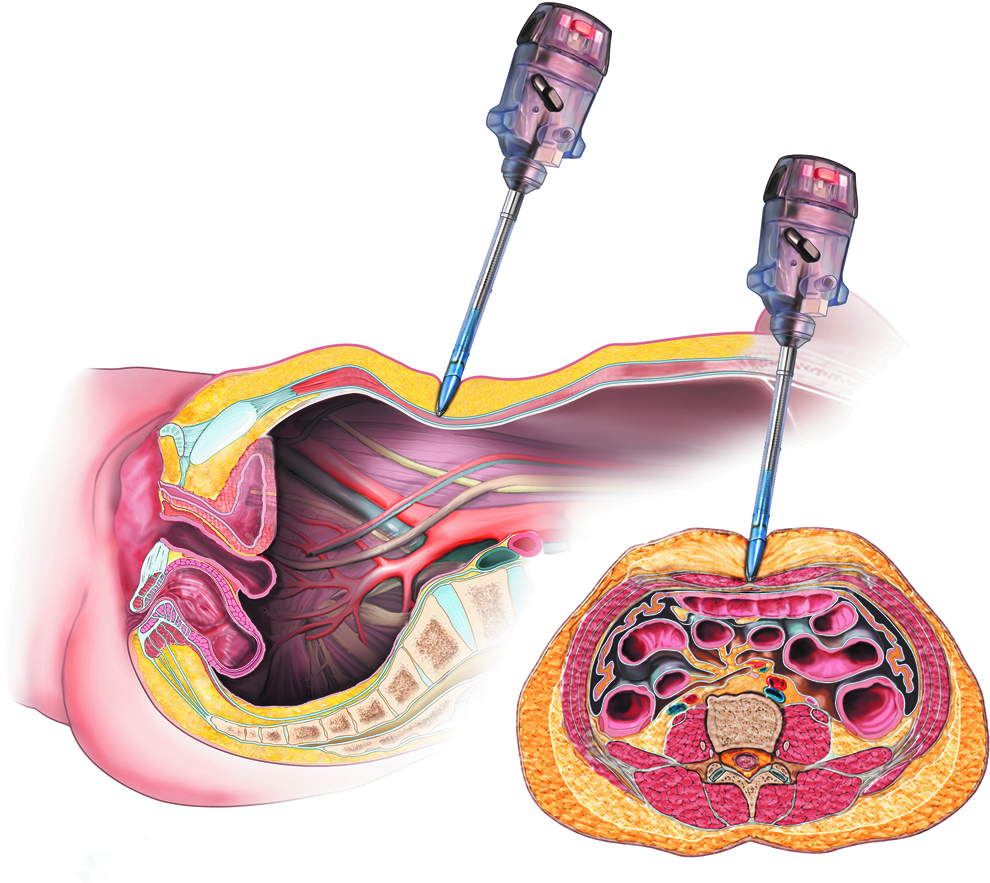
As the trocar force is applied, the obese anterior abdominal wall dislocates inward toward the vertebral column for a greater distance, thereby reducing the distance between the incursion of the anterior wall and the posterior retroperitoneum (Fig. 2). A second study published by Hurd et al. 12 focused on the relative position of the umbilicus to the aortic bifurcation. This article is frequently quoted or misquoted by proponents espousing a 90° primary trocar insertion for women with BMIs >25 (i.e., the overweight/obese range).

The obese abdomen has greater elasticity, compared to the anterior abdominal wall shown in Figure 1. Applying a trocar force pushes the wall deeper into the peritoneal cavity and encroaches on the limited space separating it from the great retroperitoneal blood vessels overlying the vertebral column.
The results of the Hurd et al. study 12 were based on retrospective, static CT scans that were not done during actual laparoscopy. A total of 35 CT scans were studied; 15 women had BMIs <25, 10 women had BMIs >25 but <30, and 10 women had BMIs >30. In the overweight and obese categories, the mean umbilical locations were 2.4 cm and 2.9 cm caudal to the aortic bifurcation, respectively. In the non-obese category, the locations of the umbilicus to the aortic bifurcation were 0.4 cm caudal in 7/15, cranial in 5/15, and at the bifurcation in 3/15. When combining the last two locations, 53% with BMIs < 25 demonstrated the umbilicus to be at or above the point of aortic bifurcation. More significantly, in the combined overweight/obese categories, the umbilicus was located at the point of aortic bifurcation in 6/20 (30%) of women.
The Hurd et al. study 12 did produce an often-overlooked fact: The relationship of the umbilicus to the left common iliac vein was always cephalad not caudal. Clearly, the content of that study should be interpreted cautiously. The statement that a 90°-trocar thrust at umbilicus is “safe”—based on the ideas that the umbilical site is caudal or below the aortic bifurcation and that the distance to the aorta from the umbilicus is >10 cm—is not correct. The “safe” interpretation is not supported by the current study or, for that matter, by Hurd et al.'s own study. 12 In the current study 78% of the women who sustained major vessel injury were in the overweight/obese BMI category. The greater thickness of the abdominal wall did not, in fact, provide discernable protection for these obese women. Finally, the most dangerous aspect of a 90° umbilical entry, as noted in the Hurd et al. 12 report, is the fact that injury to the left common iliac vein is a major risk for such an entry technique in all BMI categories.
Collateral injuries, as reported in the results section of the current article, were responsible for serious add-on injuries. In order to reduce the risk of missed second or even third vascular injuries, a missed bowel perforation, and/or a missed transected ureter, a thorough and systematic inspection of the peritoneal cavity and retroperitoneum must be carried out. Following vein injury and repair, the risks of thrombosis and compartment syndrome are increased. With massive hemorrhage, clotting factors must be replaced if coagulopathy is to be avoided. Fresh frozen plasma should be administered along with packed red-cell transfusions, and platelet/cryoprecipitate should be infused based on laboratory feedback.
Although the majority of entry injuries described in this article were trocar-related, a few were caused by a Veress needle. The Veress needle measures 12.5 cm from hub to terminus and 17.5 cm in total length. At the umbilicus, where less fat is deposited such length is excessive and unnecessary. In the early days of laparoscopy (1968) a Tuohy epidural needle was the instrument of choice for insertion and creation of a pneumoperitoneum (Fig. 3). In contrast to the Veress needle, the Tuohy needle measures 8.5 cm from tip to hub (Fig. 4). During these early times, the Tuohy needle was used for any and all patient body configurations including very obese patients.

Two needles are shown for comparison. Above is the shorter, “hockey-stick” shaped Tuohy needle; below, the longer Veress needle is shown.

The Tuohy needle, from tip to hub, measures 8.5 cm. This device enables peritoneal entry at the umbilical site even for very obese women.
If periumbilical trocar entry cannot be accomplished using a trocar insertion angle of 45°–60°, then an alternative site should be considered (i.e., the left upper quadrant in the mid-clavicular line). Another entry alternative utilizing a mini-umbilical incision and the open (Hasson) technique is safe and effective. Once a pneumoperitoneum has been established over-inflation with pressures of >20 mm Hg may provide some protection against too-deep trocar insertion. Radial expanding devices slip over a Veress needle to gain entry. Once the pneumoperitoneum is established, a blunt trocar dilates the sheath after the Veress needle is removed.
Conclusions
Major vessel laceration is a peculiar operative complication uniquely associated with laparoscopic surgery. Prior researchers have reported that this rare problem occurs with a range of 0.1–6.4 per 1000 patients and a mean incidence of 0.5 per 1000 laparoscopic procedures.13–17
Furthermore, this current study, together with other studies, demonstrated that major vessel injury is, in fact, a preventable complication.18,19 Damage to the great retroperitoneal vessels cannot occur during the entrance phase of laparoscopy unless the entry device is placed through the umbilicus at a 90° angle coupled with poorly controlled deep penetration. The vessels at risk are predominately the aorta and left common iliac vein. When the two abovementioned mistakes are coupled with misdirection of the entry instrument to the right of the midline, the vessels at risk are the right iliac arteries and veins or the inferior vena cava. When the deviation is to the left, the target vessels at risk are the left iliac arteries and veins. The prudent gynecologic surgeon can avoid this calamity by taking care to place the entry needle or trocar at a 45°–60° angle or by selecting a different entry site or technique.
Author Disclosure Statement
No competing financial interests exist.