
Abstract
Abstract
Introduction
P
A case of PSTT can be incorrectly diagnosed, as retained portions of the placenta, placenta accreta/percreta, choriocarcinoma, quiescent GTD, exaggerated placental site, placental-site nodule, or an epithelioid type of leiomyosarcoma. 4 This article reports on a case of a patient with extensive vaginal bleeding who was diagnosed with placenta accreta mimicking PSTT with the same laboratory and clinical findings. Written consent was obtained from the patient and her husband for publication of this case report.
Case
A 37-year-old patient (gravida 2, para 1) presented with abnormal vaginal bleeding. Her medical history indicated an uncomplicated first pregnancy, the product of in vitro fertilization with caesarean-section (C-section) delivery, and a complicated second pregnancy, the product of another in vitro fertilization, which had been terminated in the 15th gestational week because of membrane rupture 1 month prior to admission. The patient had been evaluated with a gynecologic examination, and dilatation-curettage was subsequently performed for supposed retained products of conception. After this procedure, the patient was discharged.
Three weeks after the first admission, the patient presented again with continued heavy vaginal bleeding. A bimanual examination revealed an enlarged uterus that was not similar to the examination 3 weeks previously. A Doppler ultrasonographic examination (General Electric Logiq S6,® 1.5–4.5 MHz probe, Waukesha, WI) revealed the presence of a heterogeneous solid mass that was 5.5 × 6 centimeters in diameter, with a high-velocity peripheral vascular pattern and markedly increased vascularization, in the uterine cavity (Fig. 1A). The patient's free ß-human chorionic gonadotropin (ß-hCG) level was 328 international units (IU)/L, and this level persisted for 3 weeks. Endometrial sampling was not performed because of the hypervascularization of the mass.
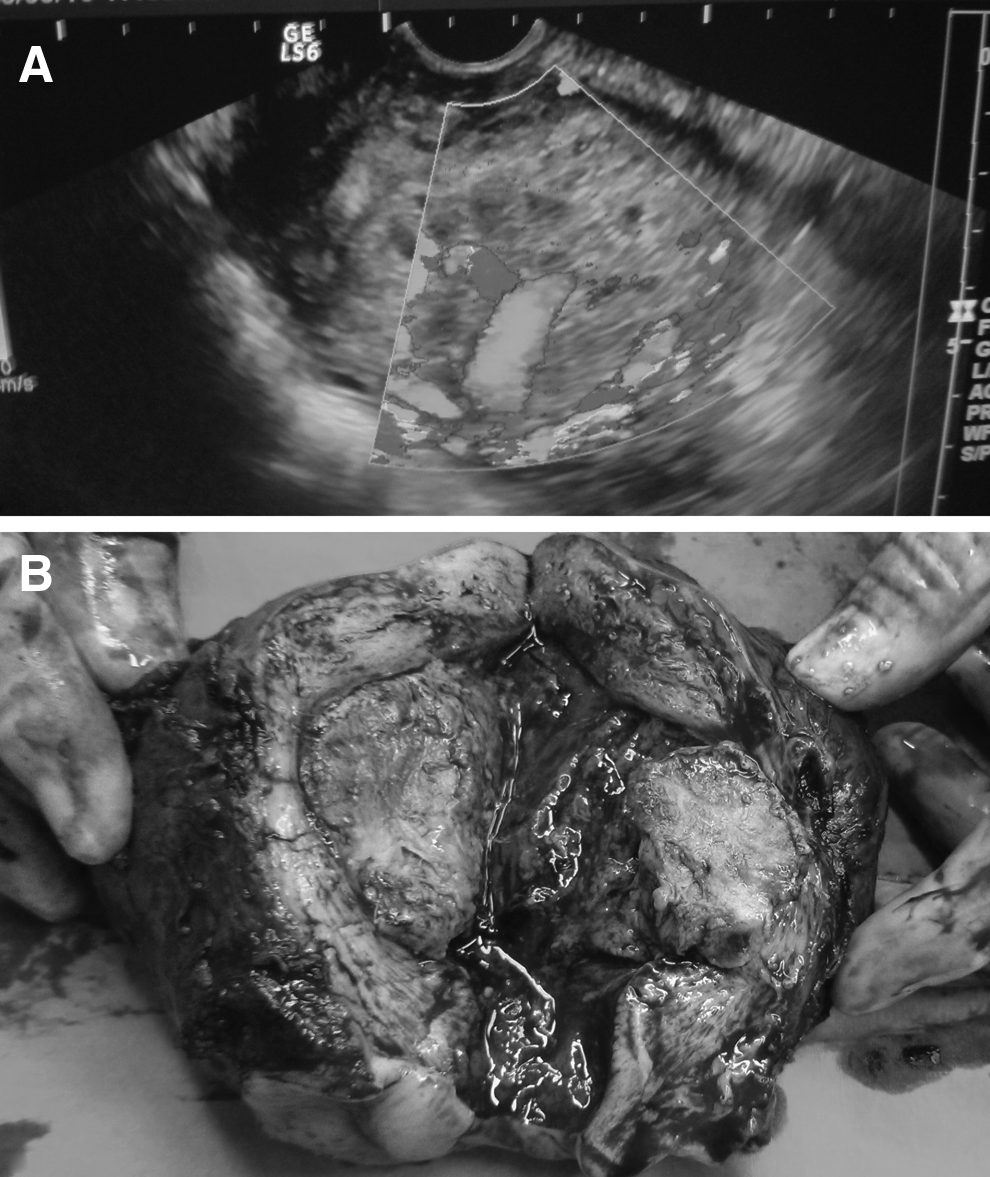
Hysterectomy was performed, with a preliminary diagnosis of PSTT. Her uterus weighed 265 g (Fig. 1B). Examination of intraoperative frozen sections of the hysterectomy material revealed that the mass was negative for malignancy. A morphologic examination showed that the placenta was attached to the previous C-section scar. The myometrial thickness at this side was 4.7 mm and was 9.8 mm at the posterior wall. The placental tissue was 1.6 mm deep in the myometrium. A histopathologic examination of the tissue sections of the basal plate of the placenta revealed the presence of myometrial fibers to which chorionic villi were firmly attached (Fig. 2). No absolute findings defining adenomyosis were evident. The morphologic and histopathologic findings of the mass were consistent with placenta accreta.
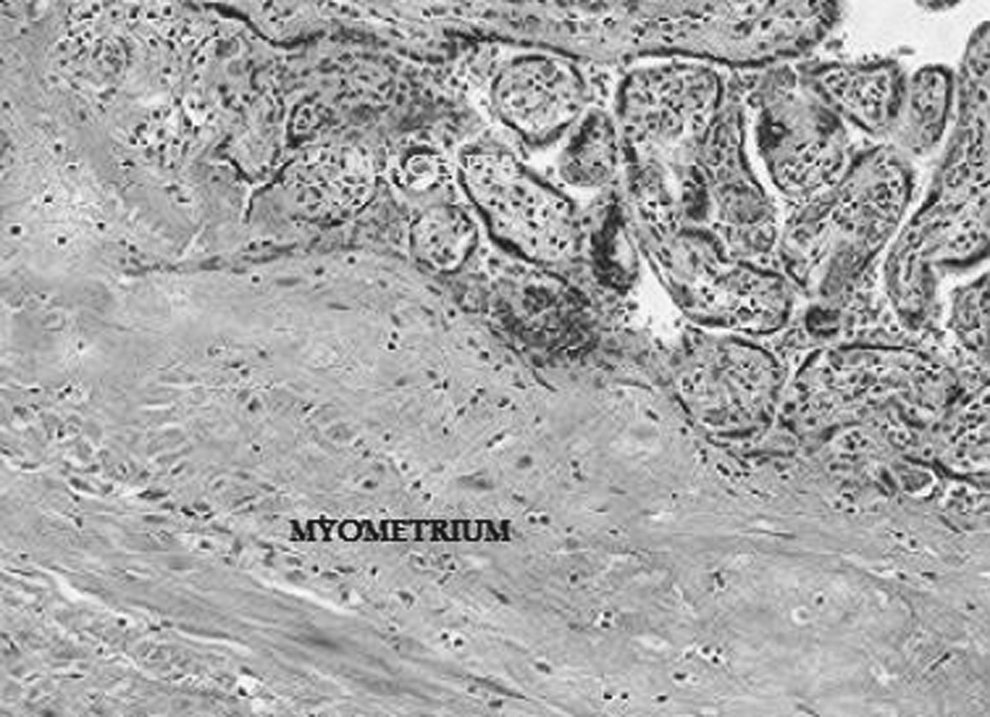
Chorionic villi were attaching focally and directly to the myometrium layer (hematoxylin and eosin × 100).
The patient was discharged at 54 hours after the surgery with no complications.
Discussion
Invasive placenta is a life-threatening condition caused by abnormal placental adherence to the uterine wall as a result of a defect in, or absence of, Nitabuch's layer. 5 The incidence of placenta accreta is reportedly lower in second trimester than in third trimester deliveries, and the condition can remain undetected in early pregnancies. 6 Findings of abnormal placental adherence on ultrasonography include the absence of a normal retroperitoneal clear zone, the presence of intraplacental lacunar spaces, and retroplacental myometrial thickness. 7
PSTT is a gynecologic tumor that takes the form of a hydatidiform mole (complete or partial), an invasive mole, or a choriocarcinoma, and originates from the trophoblast layer, making it a GTD. 2 It is a rare tumor that mainly occurs in women with histories of abortions, pregnancy terminations, or even pathologic or normal ongoing pregnancies. It appears sonographically as heterogeneous echogenic lesions, with peripheral vascular signals indicative of neoangiogenesis.1,8 A persistently low or normal ß-hCG level is helpful for the diagnosis, 8 as other forms of GTD typically have high levels of ß-hCG secretion. 9 The preliminary diagnosis was PSTT because of the similarity of the current patient's sonographic and laboratory findings to those reported in the English medical research literature.
In this current case, a malignant process such as PSTT, as opposed to placenta accreta, was indicated by the gestational week of termination (second trimester), the enlarged uterus, and the hypervascularization of the uterine mass, in addition to the uterine-wall invasion. Endometrial curettage was not performedbecause this procedure—in cases of PSTT, as well as in cases of placenta accreta—may result in heavy uterine bleeding that necessitates an emergency hysterectomy. Generally, hysterectomy is the first-choice treatment for placenta accreta as well for PSTT. 5
Cases of PSTT, as mentioned above, can be incorrectly diagnosed, based on sonographic and laboratory findings, as retained portions of placenta, placenta accreta/percreta, choriocarcinoma, quiescent GTD, exaggerated placental site, placental-site nodule, or epithelioid type of leiomyosarcoma. 4 After hysterectomy, a definitive diagnosis can be established by histopathologic examination. 10
The current authors have determined some histopathologic differences between PSTT and placenta accreta that are helpful for avoiding misdiagnosis. These include the attachment of chorionic villi to myometrial smooth-muscle fibers, the absence of—or reduction in—the decidua basalis layer with a thick layer of fibrin, and hemosiderin-laden macrophages. These three features are usually seen with placenta accreta on microscopy examination. 11 In contrast, histopathologic examination of PSTT reveals intermediate trophoblast proliferation that invades the myometrium deeply in large nests and an interdigitating pattern or masses with no cytotrophoblast and villi. Extensive deposition of fibrinoid material, with invasion of blood vessels, is usually seen in microscope images. 12
Conclusions
The rising rate of C-sections suggests that obstetricians will see more placental-attachment abnormalities. This emphasizes the importance of paying attention to the diagnosis of retained placenta accreta in patients with extensive bleeding, either postpartum or following termination or abortion. Both PSTT and placenta accreta are treated by hysterectomy, so the current authors believe that performing endometrial curettage is critical for supporting a prediagnosis, which, in both diseases, could result in prolific bleeding. The aim in presenting this case is to call attention to known similar laboratory and sonographic findings between placenta accreta and the rare malignant PSTT tumor, as well as to show that misdiagnosis between them can be rectified with a histopathologic examination.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests. The authors also declare that work on this case report did not receive any financial support.