
Abstract
Abstract
Introduction
V
Case
A 51-year-old female underwent total laparoscopic nerve-sparing radical hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymph-node dissection, for cervical squamous cell carcinoma, International Federation of Gynaecology and Obstetrics stage1B2. Final pathology testing revealed pT2bN0M0 with invasion of the left parametrium. It was recommended that she receive concurrent chemoradiation therapy 8 weeks after the surgery. Radiation therapy to the pelvis was delivered daily for 5 weeks with concurrent chemotherapy (a weekly bolus of 40 mg/m2 of cisplatin), which was started on day 1 of radiotherapy for 5 times.
Three months after this concurrent chemotherapy, VCD with small-bowel at the vaginal opening was observed via a speculum examination, at the outpatient clinic on her regular follow-up (Fig. 1). This patient was asymptomatic. There were no signs of incarceration and infection. It was decided to wait for spontaneous vaginal closure and to reassess the condition of her vagina every 3 months.

Portion of small bowel entrapped into the vaginal cuff dehiscence seen on speculum examination (54 × 40 mm).
Results
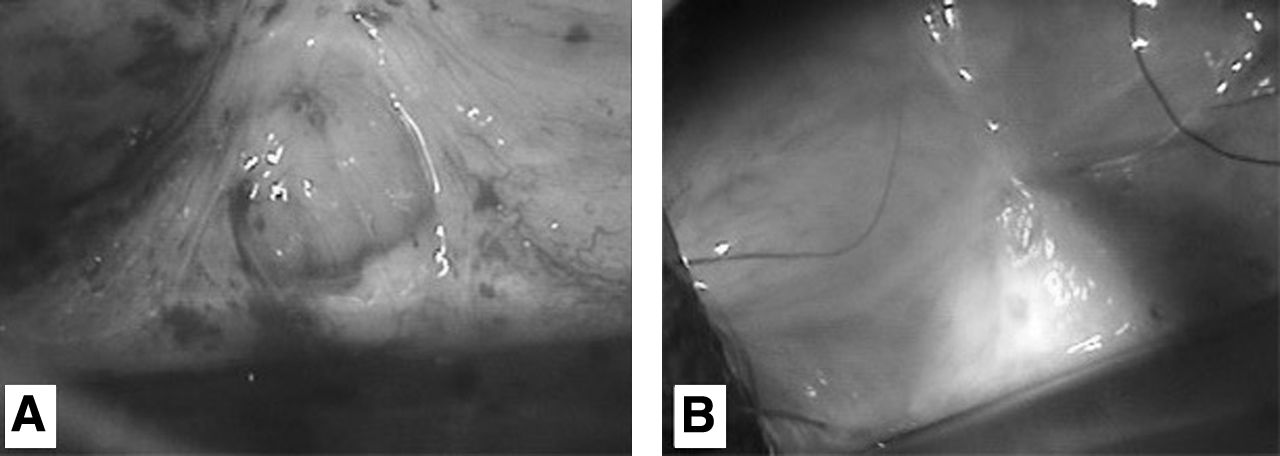
Three months after her VCD diagnosis, this patient's vaginal opening became smaller and was already covered by a thin membrane. This membrane gradually became thicker and the vaginal opening was completely closed after 2 years. (Fig. 2A and B) She receives follow-up examinations regularly without recurrences noted as of this writing.
Discussion
VCD is a rare but severe morbidity following hysterectomy. Although the rates of VCD are different from study to study, robotic and laparoscopic hysterectomies have higher rates of VCD (ranges: 0.64%–4.1%, 0.47%–4.93%, respectively) than vaginal and abdominal hysterectomies (ranges: 0.13%–0.29%, 0.12%–0.99%, respectively).3,4 This surgical risk factor is more associated with minimally invasive approaches because of the use of electrosurgery for colpotomy that is said to impair wound healing. 4 However, Fanning et al. reported that the vaginal closure technique plays a role in the increased VCD rate associated with total laparoscopic hysterectomy, not the electrosurgery. 5 Smoking, diabetes, chronic lung disease increasing intra-abdominal pressure, vaginal atrophy, advanced age, chronic steroid use, postoperative radiation therapy, sexual intercourse before healing, postoperative cuff infection, and hematomas are also associated with VCD.
In the current case, the risk factor associated with VCD was the use of electrosurgery for colpotomy and the postoperative radiation therapy given to the patient. There were no symptoms of infection and no history of sexual intercourse. Radiation therapy may impair wound healing and be the cause of VCD. Radiation disrupts the inflammatory, proliferative, and remodeling phases of wound healing and reduces nitric oxide, which promotes wound healing by induction of collagen deposition. 2 This results in pathologic fibrosis and its complications, such as strictures and fistulae of the vagina, and can affect surgical outcomes of VCD.
Articles relevant to
The current patient had a complete disruption of the vaginal cuff with bowel evisceration. In the current authors' experience, the bowel has been viable with active peristalsis and there have been no ischemic injury, peritonitis, or sepsis. Thus, it was decided to await spontaneous healing of this patient's vagina.
Cronin et al. performed a review of original research, case reports, and case series published in the past 30 years on VCD. 4 These researchers reported that 5% of patients were allowed to heal by secondary intention after VCD or evisceration. Of the 73 cases of dehiscence that were found in that review, 3 patients (4%) each had another dehiscence that required a second repair. So, the higher rate of another dehiscence following radiation therapy was considered.
Conclusions
As most gynecologists noted in their reports, surgical repair was used to treat VCD. However, case reports on VCD occurring after radiation therapy are scarce. It may take time to heal a surgical wound completely following radiation therapy as shown in the figures (Figs. 1 and 2). However, in cases with rigid vaginal mucosa post radiation therapy or in patients with previous polysurgery wherein another surgery— either vaginal or abdominal—would be risky, nonclosure can be another option for approaching VCD. Otherwise, the most important thing is that one has to evaluate the patient's general condition to decide proper management of that individual patient's VCD.
Footnotes
Acknowledgments
The authors thank The Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital for Dr. Soshi Kusunoki.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.