
Abstract
Abstract
Introduction
T
Case
A woman in her mid-70s presented with a perineal mass. After biopsy confirmation of the diagnosis, she underwent wide local excision of a 6.0 × 5.0 × 3.0 cm solid mass. The lesion came within 2 mm of the resection margin, and showed lymph vascular space involvement. Thus, she was subsequently referred for radiation therapy.
Results
Pathology testing showed that the multinodular yellow–tan lesion had eroded through the surface epithelium (Fig. 1). Histologically, the tumor was composed of nests and sheets of poorly differentiated epithelial cells (Fig. 2). At the periphery of the tumor, a spray pattern of keratinizing infiltrating eccrine ducts (Fig. 3) confirmed the diagnosis of SEC.

Excision specimen showing lesion ulcerating through skin.
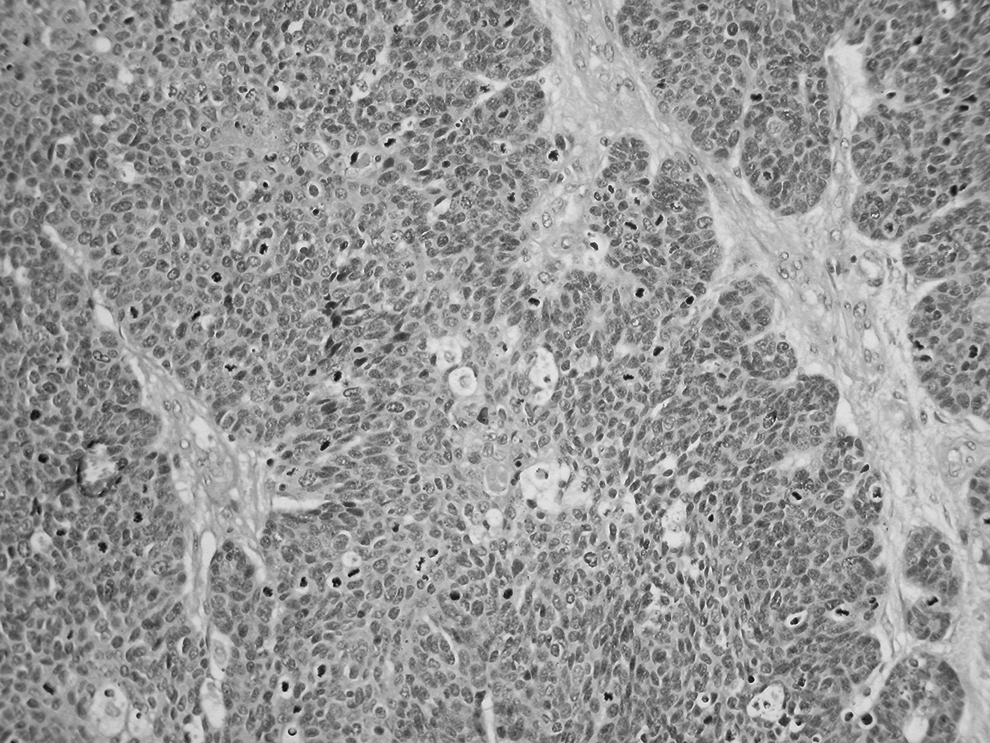
Much of the tumor was composed of sheets and nests of poorly differentiated cells
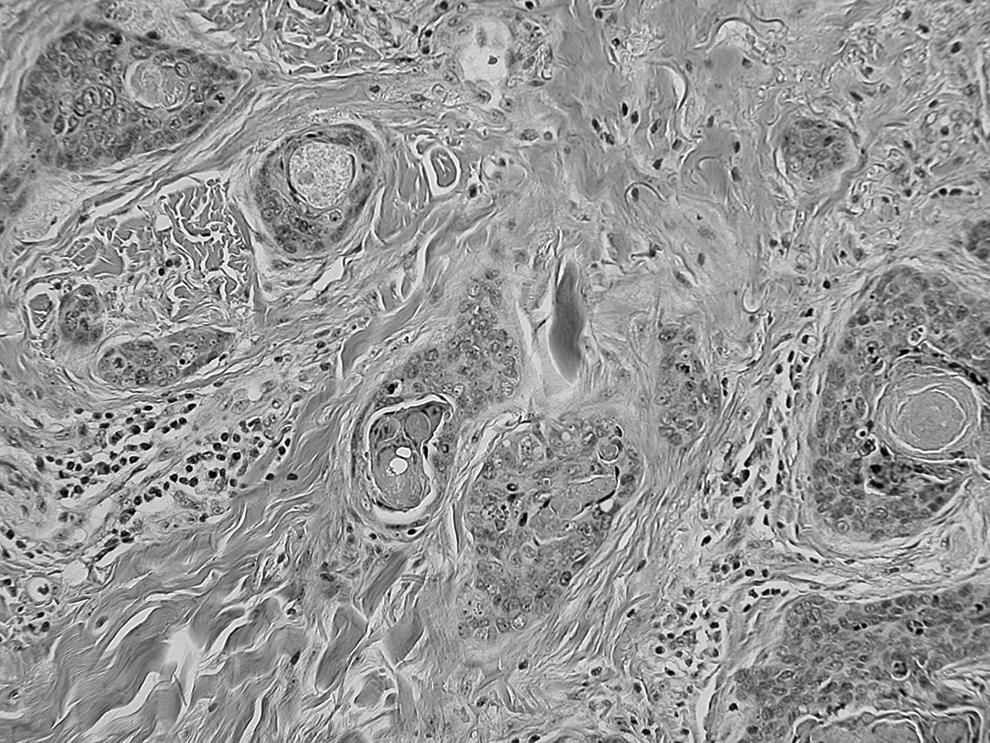
At the edge of the lesion, there was a spray-like pattern of infiltrating keratinizing syringomatous ducts.
Discussion
Skin adnexal neoplasms of the vulva are uncommon, and malignant adnexal neoplasms of the vulva are rare. 2 Classification of malignant sweat-gland neoplasms is somewhat confusing, but, to some degree, parallels that of their benign counterparts. Hence, this tumor (SEC) is parallel to benign syringoma with respect to categorization. SEC is also known by a variety of other names, including eccrine carcinoma and syringomatous carcinoma, among others. Benign syringomas occasionally occur on the vulva, although they occur more often on the face and present as multiple pruritic flesh-colored papules. SEC resembles syringoma in the formation of comma-shaped ductal structures but also has features of malignancy, including cellularity and invasiveness. 2
SEC was first described in 1969, 3 and this rare neoplasm is reported predominantly on the scalp, head, neck and trunk,4,5 with only 1 other case on the vulva reported. 2 The lesions do not have a characteristic or consistent immunohistochemical profile. 5 SECs are locally aggressive, with a tendency to recur,2,4 and lymph-node involvement and distant metastatic disease occur occasionally.4,5 There are no well-established protocols for treating this rare lesion; the primary treatment is excision. The role of lymph-node dissection is controversial, with recommendations including regional node dissection for clinically positive nodes for vulvar sweat-gland carcinomas, 6 and ipsilateral node dissection for vulvar sweat-gland carcinomas, without specification of SEC. 7 Of interest is a report of eccrine carcinoma of the vulva associated with extramammary Paget's disease. Although not called syringomatous, one of the images in this article does have features suggestive of this diagnosis. 8
In the current case, the proximity of the tumor to the margin and lymph vascular space involvement led to the recommendation for adjuvant radiotherapy.
Conclusions
The potential for nonsquamous malignancy of the vulva should be considered when patients present with vulval lesions, and liberal biopsy of all lesions of the vulva should be performed.
Footnotes
Author Disclosure Statement
No financial conflicts exist.