
Abstract
Abstract
Introduction
S
The goal of NOTES is to reach the abdominal cavity by scar-free means, thus surgical procedures are performed via a natural body orifice. In recent years, these techniques have gained popularity among general surgeons, gynecologists, urologists, and gastroenterologists; and their feasibility and safety have now been accepted. 3
The stomach, esophagus, bladder, and rectum all provide adequate NOTES access points, but the majority of NOTES procedures have been performed transvaginally. 4 The vagina provides direct access to the peritoneal cavity and can be decontaminated easily. Not only gynecologists but also general surgeons make extensive use of culdotomy for several surgical procedures and for extraction of large specimens, and it has been approved as safe and easy to close. 5
In hybrid NOTES the surgical procedure is performed through a natural body orifice with transabdominal assistance. The term pure NOTES refers to procedures that involve only transluminal access.
Hysterectomy via NOTES—after performing an anterior and posterior colpotomy and transection of the uterosacral ligaments via classical open vaginal surgery—has been described.6,7 This technique is termed vaginally assisted NOTES hysterectomy (VANH), as the first part of this procedure is performed by conventional vaginal surgery, and in the second part of the procedure, the hysterectomy is performed via NOTES (Table 1).
NOTES, natural orifice transluminal endoscopic surgery.
In a total vaginal NOTES hysterectomy (TVNH), the entire hysterectomy is performed via transvaginal NOTES. 8 In VANH, the circumcision of the cervix, the anterior and posterior colpotomy, and the ligation of the uterosacral ligaments are performed by classical vaginal surgery, whereas, in TVNH, this part of the procedure is also performed using endoscopic instruments via the NOTES approach. This enables the surgeon to perform the anterior and posterior colpotomy more easily in patients without descensus, in those who have not delivered vaginally, and in those with previous caesarean sections. 8
The first case report on transvaginal robotic surgery was presented at the Society of European Robotic Gynecologic Surgery's Meeting on Robotic Gynaecological Surgery in June 2015. 9 From the first case series of 5 patients, a new technique of robotic vaginally assisted NOTES hysterectomy (RVANH) was published. 10 RVANH makes use of the advantages of robotic surgery to broaden the indications for vaginal hysterectomy and can help overcome its limitations, while the NOTES approach avoids abdominal-wall wounds and trocar-related complications. 10
Previous experience with TVNH and with transvaginal robotic surgery for RVANH led to the decision to combine these techniques to perform robotic total vaginal NOTES hysterectomy (RTVNH) in nulliparous patients.
Materials and Methods
Patients
A single surgeon (J.B.) performed 20 robotic transvaginal NOTES (VNOTES) hysterectomies: 10 TVNH on nulliparous patients and 10 VANH on parous patients. In the RTVNH group, 7 patients were operated for myomatous uterus, 2 for cervical dysplasia, and 1 for Stage IA endometrial cancer. In the RVANH group, 5 patients were operated for Stage IA endometrial cancer and 5 patients for myomatous uterus.
Patient selection criteria included: no contraindication for general anesthesia, pneumoperitoneum or Trendelenburg position; no fixed uterus, strong pelvic adhesions, or nodularity in the pouch of Douglas on clinical examination; no history of pelvic inflammatory disease. Obesity (BMI >30) was not considered to be an exclusion criterion.
The following patient and perioperative data were collected and analyzed retrospectively for each patient: age; body mass index (BMI); parity; mode of delivery; previous surgery; type of surgery; operating time; serum hemoglobin (Hb) drop (change between preoperative Hb and postoperative Hb, 1 day after surgery); perioperative complications; postoperative pain score, hospitalization time; and uterus weight. The time from placement of the Foley catheter to completion of vaginal closure was taken as the duration of surgery. Intraoperative complications included bowel, bladder, ureteric or vascular injuries, as well as blood loss >300 mL. Short-term postoperative complications included postoperative ileus, vaginal-vault bleeding or infection, urinary tract infection, or hematuria.
A visual analogue pain scale (VAS; scoring from 0 = no pain, to 10 = worst imaginable pain) was used postoperatively to assess pain. It was evaluated at 6 and 24 hours postoperatively. Intravenous (i.v.) paracetamol (1000 mg) and ketorolac trometamol (20 mg) were administered intraoperatively to all patients. Postoperatively, pain was managed by paracetamol (1000 mg) and ketorolac trometamol was administered per each patient's demand.
Prophylactic i.v. antibiotic therapy—cefazolin (2 g) and metronidazole (500 mg)—was administered during surgery.
Patients were instructed that no vaginal intercourse was allowed for 6 weeks after the procedure. Each patient was reassessed at a postoperative consultation 6 weeks after surgery.
Surgical technique
RTVNH was performed in 10 nulliparous patients. A NOTES port was constructed by assembling a surgical glove, a wound protector, 4 Da Vinci 8-mm trocars, and 1 reusable 5-mm trocar (Fig. 1). The ring of the wound protector was then inserted into the vagina to create a pneumovagina. A Da Vinci Xi surgical robot was side-docked between the legs of each patient. Three arms were connected to the trocars in the gloveport. The fourth arm was not used. Using a 30° optic, a fenestrated bipolar grasper, and monopolar scissors, the hysterectomy was performed via transvaginal NOTES using the surgical robot (Fig. 2). The fallopian tubes were removed with the uterus after bipolar cauterization and transection of the ovarian ligament. When indicated, the ovaries were removed by bipolar cauterization and transection of the infundibulopelvic ligament. Once the hysterectomy was completed, the robot and gloveport were removed. When the uterus was too large to extract in toto, it was morcellated manually so that it could be removed vaginally. The colpotomy was closed as in classical vaginal surgery. No abdominal incisions were made.

A natural orifice transluminal endoscopic surgery (NOTES) port was constructed by assembling a surgical glove, a wound protector, 4 Da Vinci 8-mm trocars, and 1 reusable 5-mm trocar.
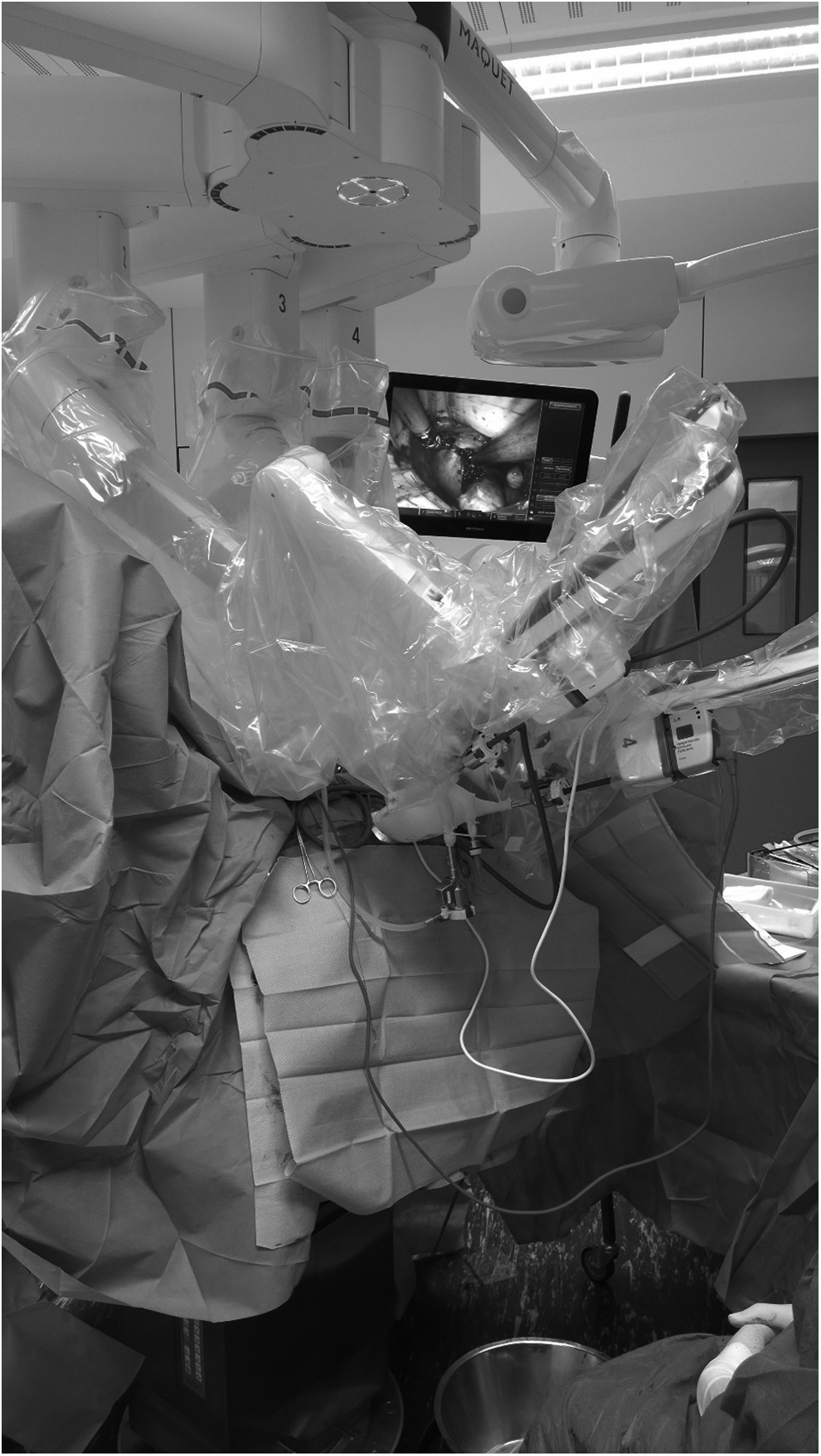
A Da Vinci Xi surgical robot was side-docked between the legs of each patient.
RVANH was performed in 10 parous patients. Each patient was placed in the lithotomy position as for a classical vaginal hysterectomy. Circumcision of the cervix, opening of the anterior and posterior peritoneum, and transection of both uterosacral ligaments was performed by classical vaginal surgery. A NOTES port was constructed by assembling a surgical glove, a wound protector, 4 Da Vinci 8-mm trocars, and 1 reusable 5-mm trocar. The ring of the wound protector was then inserted transvaginally into the peritoneal cavity to create a pneumoperitoneum. A Da Vinci Xi surgical robot was side-docked between the legs of each patient. Three arms were connected to the trocars in the gloveport. The fourth arm was not used. Using a 30° optic, a fenestrated bipolar grasper, and a vessel sealer, the hysterectomy was performed via transvaginal NOTES using the surgical robot. The fallopian tubes were removed with the uterus after transection of the ovarian ligament by vessel sealer. When indicated, the ovaries were removed after transection of the infundibulopelvic ligament by vessel sealer. Once the hysterectomy was completed, the robot and gloveport were removed. When the uterus was too large to extract in toto, it was morcellated manually so that it could be removed vaginally. The colpotomy was closed as in classical vaginal surgery. No abdominal incisions were made.
Results
Twenty robotic VNOTES hysterectomies were performed successfully. No conversion to standard multi-incision laparoscopy or laparotomy was necessary.
Table 2 presents an overview of patient and perioperative data. Individual patient details are presented in Table 3.
BMI, body mass index; min, minutes, RVANH, robotic vaginally assisted NOTES hysterectomy; RTVNH, robotic total vaginal NOTES hysterectomy; NOTES, natural orifice transluminal endoscopic surgery.
min, minutes; LLETZ, large loop excision of transformation zone; AE, appendectomy; CS, cesarean section; USO, unilateral salpingo-oophorectomy; NOTES, natural orifice transluminal endoscopic surgery; RTVNH, robotic total vaginal NOTES hysterectomy; BSO, bilateral salpingo-oophorectomy; CABG, coronary artery bypass graft; LS, laparoscopic sterilization.
In the RTVNH group, the mean age was 49 (range: 40–73), mean BMI was 26.4 (range: 20.5–40.2), mean procedure time was 118 minutes (range: 75–165), mean Hb drop 1.2 (range: 0.7–2.5), mean VAS score on day 1 was 2 (range: 1–3), and on day 2 was 2 (range: 1–2), and the mean uterus weight was 149 g (range 21–518). No complications occurred.
In the RVANH group the mean age was 63 (range: 46–84), mean BMI was 27.8 (range: 21.2–37.9), mean procedure time was 90 minutes (range: 56–120), mean Hb drop 1.3 (range: 0.5–2.6), mean VAS score on day 1 was 2 (range: 2–3), and on day 2 was 2 (range: 1–2), and the mean uterus weight was 213 g (range 70–575). One patient developed a superficial thrombophlebitis postoperatively.
Each patient was examined 6 weeks after surgery. There were no vaginal wound infections nor dehiscences, and none of the patients complained of pain during pelvic examinations. All patients were in good health and back at work.
Discussion
These 20 cases of robotic VNOTES hysterectomy were performed successfully. The procedures were completed within a reasonable operation time and without major complications. No conversion to laparotomy, transabdominal robotic surgery, or standard laparoscopy was necessary. The duration of hospitalization was similar to that for a laparoscopic or vaginal hysterectomy in the current author's department.
To the best of the current author's knowledge this is the first report on RTVNH. As the Da Vinci Xi surgical robot is designed for multiport access, the surgical team experienced significantly more robotic-arm collision during these transvaginal NOTES procedures than was normally experienced during multiport transabdominal procedures. Particularly, in the final stage of the hysterectomy, the arms had to be repositioned more frequently. Having longer robotic instruments and narrower robotic arms would have facilitated this part of the procedure better. Overall, the arm collision problem was similar in the RTVNH and RVANH groups, and was smaller than we had anticipated.
Compared to laparoscopic surgery, conventional transvaginal surgery has significant advantages, such as the absence of abdominal scarring and faster recovery from surgery. 11 Conventional transvaginal surgery is the preferred approach to hysterectomy. 12 Vaginal hysterectomy can be performed safely in patients with large uteri 13 and in nulliparous women. 14 The risk of complications, however, is higher in nulliparous women. 14 The accessibility of the vaginal passage, disease confined to the uterus, and the surgeon's experience are the major determining factors for the choice of route of hysterectomies. 15
Over the last years, the incidence of robotic hysterectomy and laparoscopic hysterectomy has increased and the incidence of vaginal and abdominal hysterectomy has decreased. 16 Enlarged uteri, undescensus, or restricted vaginal space in nulliparous women present certain challenges when using conventional vaginal hysterectomy techniques. 7 The technical drawbacks of transvaginal surgery—which include limited visualization to attempt good hemostasis and difficulty in performing adnexectomy in case of adhesions between the adnexa and the uterus—can be overcome by performing transvaginal NOTES.8,10 In addition, the risk of trocar-related complications is eliminated by NOTES and postoperative pain is reduced. 17 It has been demonstrated that very large uteri can be removed using VANH, and that ligating the uterine vessels transvaginally before dissecting the rest of the uterus results in less blood loss, compared to what occurs with a transabdominal laparoscopic approach, wherein there is more manipulation before occlusion of the feeding vessels.6,7
RTVNH and RVANH are two novel techniques requiring further validation. When comparing both patient groups that mainly differed in parity, the results were similar. The operating time for RTVNH was longer than for RVANH, which is also the case when comparing TVNH with VANH in the current author's experience. RTVNH enabled the current author's surgical team to perform hysterectomies without any abdominal incisions in nulliparous patients, who were assessed not to be candidates for classical vaginal hysterectomy. However, from previous experience, it can be concluded that this could also have been achieved by TVNH.
The major advantages of robotic surgery over laparoscopic surgery are better ergonomics and better camera control and articulated wrist motion. When comparing RTVNH and RVANH with the current author's surgical team's previous experience with VANH and TVNH, the team was able to confirm these advantages. However, the total operating time was significantly longer in RTVNH and RVANH, compared with the team's experience with VANH and TVNH. Further technical innovations in surgical robots will help overcome the problem of robotic-arm collision and will therefore reduce the time of surgery. The inability, during VNOTES, to overview the pelvic area—in particular, the vesicouterine pouch—is a major limitation that could lead to lesions, such as bladder endometriosis, being missed. Innovation of endoscopes is desirable to overcome this limitation and to have the ability with NOTES to explore the entire abdominal cavity. 18 As with all robotic surgery the cost of an RTVNH will need to be assessed in comparison to the advantages it provides over a TVNH or a total laparoscopic hysterectomy.
Pelvic infection after vaginal surgery could present a possible argument against RTVNH or RVANH; however, no patient in this study had such a complication. Previous studies have also shown that postoperative pelvic infection is unlikely, especially when prophylactic antibiotics are administered.7,19 To prevent ureteric damage, the uterus is pushed cranially and medially with a robotic fenestrated grasper. Closure of the vaginal vault follows the same technique as in a classical vaginal hysterectomy; thus, no differences in incidence of dyspareunia are to be expected. Sexual abstinence should be recommended for 6–8 weeks, as is the recommendation for conventional transvaginal surgery. 7
The current author's surgical team follows the principles of the IDEAL [Innovation, Development, Exploration, Assessment, and Long-term study] paradigm for their surgical research. 20 This paradigm states the importance of scientific reporting on procedures in stage 1. The current study describes two procedures in stage 1 according to IDEAL principles. Therefore, the number of patients is small and the type of patients is highly selective. The output is descriptive. The intervention is a procedure inception and the outcome is proof of concept. It is important to emphasize that the results of a stage 1 study can never demonstrate superiority of a new surgical technique over an existing technique. Conventional transvaginal surgery remains the preferred approach to hysterectomy, and nulliparity is not a contraindication for a conventional vaginal hysterectomy. It is important to continue researching on robotic VNOTES surgery, as it potentially combines both the advantages of robotic surgery and of NOTES surgery. The NOTES approach offers better visualization and better access for removing the fallopian tubes (and ovaries). NOTES also uses the advantages of endoscopic surgery to broaden the indications for vaginal hysterectomy and helps overcome its limitation. Robotics adds improved ergonomics as well as better camera control and articulated wrist motion.
Patients in IDEAL stage 1 are always carefully selected; therefore, the uterus sizes in this study were small. Now that proof of concept has been demonstrated, further IDEAL stage 2 studies need to demonstrate the advantages of RVANH and RTVNH for removing larger uteri.
Conclusions
This case series confirmed that robotic transvaginal surgery was feasible and that it could be used to perform total hysterectomy. RTVNH is feasible and enabled the surgical team to perform hysterectomies without any abdominal incisions in nulliparous patients, who were assessed not to be candidates for a classical vaginal hysterectomy. RTVNH and RVANH make use of the advantages of robotic surgery to broaden the indications for vaginal hysterectomy and can help overcome its limitations, while the NOTES approach avoids abdominal-wall wounds and trocar-related complications. Further developments in robotic technology will help overcome the problem of robotic-arm collision. Robotic hysterectomy via vaginal access is a novel approach that requires further validation. The extra cost and set-up time of RTVNH and RVANH will also need to be assessed in comparison to the advantages they provide over TVNH, VANH, or total laparoscopic hysterectomy.
Footnotes
Acknowledgments
Thanks are extended to Ms. Amanda McPhail for language correction and editing of the manuscript for this article.
Author Disclosure Statement
The author declares that he has no conflict of interest.