
Abstract
Abstract
Introduction
T
Leiomyosarcomas (LMS) are rare, malignant aggressive tumors originating from smooth-muscle tissue. Most LMS arise de novo, while malign transformation is known but very rare. Uterine LMS have been the subject of much discussion because of cases in which suspected benign leiomyomas have been power morcellated and subsequently have proven to be LMS. Some of these cases have received public attention and have led to the U.S. Food and Drug Administration (FDA) issuing a warning against uncontained power morcellation. 2 The rate of unsuspected, morcellated LMS is estimated to be ∼0.09%. 3
Esmya® (Gedeon Richter, Budapest, Hungary; ulipristal acetate; UPA), a selective progesterone modulator, has been approved as a therapy for symptomatic fibroids. UPA seems to be an effective and safe method of treating uterine fibroids and has been shown to reduce bleeding and fibroid size. 4 Therefore, UPA is indicated for intermittent, long-term, and preoperative treatment of moderate-to-severe symptoms of uterine fibroids in adult women of reproductive age. In the present case, there was inadvertent treatment of LMS with UPA—an occurrence that the current authors were unable to find in the literature.
In order to remove large fibroid uteri laparoscopically, the uterus must be cut into smaller pieces (morcellated) for extraction. A common method of morcellation involves a technique in which an electromechanical device with a cylindrical blade circulates at high speed within a trocar to cut the enlarged specimen into narrow strips. The specimen is often morcellated within the abdominal cavity without using an enclosing trap to collect the tissue (“open” power morcellation), thus exposing the abdominopelvic cavity to disrupted tissue from the specimen. Complications from open morcellation include injury to surrounding structures, such as the bowel or major vessels, difficult histologic examination of a specimen because of the piecemeal presentation, and inadvertent dissemination of the morcellated specimen within the abdominopelvic cavity. When there is an unsuspected uterine sarcoma, this is particularly unfortunate, as this automatically leads to upstaging of the cancer to International Federation of Gynecology and Obstetrics stage IIA and worsens the prognosis.5–8
A way of avoiding disrupted tissue spreading in the abdominal cavity is by using a contained morcellation technique.9,10 Given that this issue was raised by the U.S. FDA, the current authors have used a contained morcellation technique at one of their hospitals, using different kinds of bags for this purpose.
This report presents and discusses contained power morcellation of an inadvertently detected LMS in a woman who had received treatment with UPA over a 6-month period before her total laparoscopic hysterectomy. The current authors have been unable to find similar articles addressing this issue in the literature.
Case
A 45-year-old woman was referred to a hospital in October 2015 with a symptomatic uterine fibroid. Her symptoms were heavy menstrual bleeding (HMB) and incontinence caused by pressure from the fibroid. Her previous gynecologic history included: an uncomplicated vaginal delivery in 2003; a surgical abortion in 2007; and an uncomplicated caesarean section in 2008. She did not have any history of abnormal cervix cytology.
This patient's fibroid was incidentally discovered in March 2014 on a magnetic resonance imaging (MRI) scan, which was conducted because she had lumbar pain (Fig. 1).

Magnetic resonance imaging of fibroid (unknown leiomyosarcoma) 20 months prior to hysterectomy.
At that time, the fibroid measured 7 cm. The morphology of the fibroid was not described in further detail. Previously she had HMB, and had experienced an episode of particularly heavy bleeding in February of 2015. During the late spring and summer of that year, she had several more episodes with severe bleeding and more-or-less constant bleeding between these episodes. Approximately 1 month after the MRI she was referred by her general practitioner to a private gynecology clinic to map and investigate the fibroid further. It was ultrasonically measured to 5.6 × 6 cm and was described as transmural and without suspicious signs such as abnormal color flow or lacuna of fluids. Since 2010 the patient had had a progestogen intrauterine device (IUD; Mirena,® Shering, Berlin Germany); in June of 2014 this IUD was exchanged with a new progestogen IUD. At this time; the same size fibroids were seen on ultrasound.
Because of this patient's heavy bleeding in spite of the 1-year-old progestogen IUD, she was referred again in June 2015 to a private clinic with a request to have the IUD removed. At that time, the fibroid measured 7.5 cm and no change in the structure of the fibroid was described. The IUD was removed and the woman was instead given Esmya. During this visit, she complained of having light dull pain during the afternoons and, ∼3 weeks later, she contacted the same clinic because she had increased bleeding and dull pain in relation to bleeding while still being treated with UPA. Tranexamic acid (dose unknown) was prescribed and the bleeding ceased. The gynecologist arranged a control appointment 6 weeks later to view the fibroid with ultrasound. However, this appointment was cancelled this due to cessation of the patient's bleeding and symptoms.
In late August of 2015, after the patient had been maintained on 3 months on UPA, her fibroid measured 9 cm. (Oddly, in the patient's record, the fibroid was actually described as decreased in size to 9 cm, which was rather contradictory). She reported that still experienced regular pain and needed to take acetaminophen (dose unknown) to control this. In September of 2015, she was then admitted to a gynecologic department because of increased pain. A high level of C-reactive protein (CRP) was found, and necrosis of the fibroid was assumed to be the reason. At a control appointment at the private clinic in October 2015, the option of referral to hysterectomy was discussed. She decided in December 2015 to opt for a laparoscopic hysterectomy at the hospital because of her increasing pain and pressure symptoms of the fibroid as well as a lack of conviction that the pharmaceutical therapy was sufficient. She did, however, remain on the UPA until a few days prior to the hysterectomy. During the preoperative examination, ultrasound showed a 10.6 × 7.3–cm fibroid with no abnormal blood flow or lacuna of fluid inside the fibroid. There was no suspicion of any malignancies in this patient (Fig. 2).

Transvaginal ultrasound 10 days before surgery.
A hysterectomy was initiated according to standard procedure of the hospital. With the patient under general anesthesia, a uterine manipulator (V-care,® ConMed, Utica, NY) was placed inside the uterus. Intraperitoneal insufflation was achieved using a Veress needle in the umbilicus. An intra-abdominal pressure of 12-mm of mercury was maintained throughout the procedure. A 12-mm trocar was introduced in the umbilicus and three additional 5-mm trocars were placed in the left iliac fossa, the right iliac fossa, and 6 cm above the umbilicus. Using an ultrasonic cut-and- seal device (Thunderbeat,® and bipolar instruments, Olympus, Hamburg, Germany) on the left side, the round ligament and the mesosaslpinx were dissected to remove the fallopian tubes (Fig. 3). The proper ligament of the ovary and the broad ligament were then dissected to the vesicouterine pouch, and the peritoneum was pushed toward the bladder. On the right side, where the fibroid was causing pressure, the same procedure was utilized. The uterine arteries, the cardinal ligaments, and the sacrouterine ligaments were cut close to the cervix. The vaginal vault was opened using the Thunderbeat device. After this, the vaginal vault was closed laparoscopically using a barbed suture.

Intraoperative image prior to start of surgery.
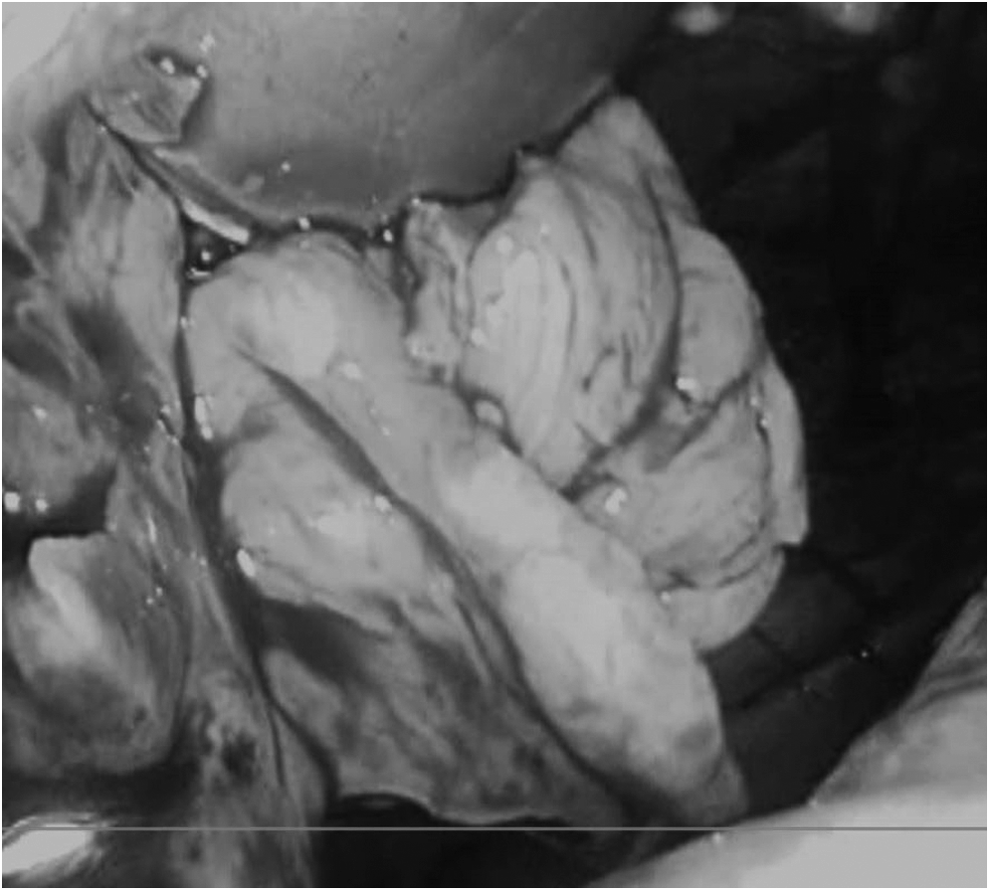
Then, a 4-L bag with a sleeve for the optic (Espiner® Medical, Clevedon, UK) was introduced through the umbilical incision (Figs. 4 and 5). The uterus was placed in the bag and the bag was insufflated to a pressure of 15 mm Hg, creating a lining of the abdominal cavity. The uterus was then morcellated, using a power morcellator of 20 mm (Wolf,® Hamburg, Germany) through the umbilical incision. The camera was inserted through the trocar in the right iliac fossa, and this was introduced through the sleeve of the bag (Fig. 6). Finally, the bag was removed and no spillage was seen. The fascia in the 12-mm umbilical incision was closed using a PDS® 0 hook suture, the skin was closed using a Monocryl® (both at Ethicon, Cornelia, Georgia) suture.

The uterus dissected and placed inside the bag before morcellation.

The bag with the sleeve for the 5-mm optic.
Morcellation with 20-mm knife of leiomyosarcoma inside the bag.
The weight of the uterus was 575 g. Histology testing showed LMS with a tumor consisting of moderately pleomorphic spindle-shaped cells with up to 18 mitoses per 10 high-power fields. The tumor was also positive for estrogen receptor–beta and partially positive for progesterone receptors.
Results
Subsequently, the patient was referred to the department of oncological gynecology, of the National Hospital in Copenhagen, Denmark. Shortly after reference to the oncology clinic, the woman had an episode of vaginal bleeding. A biopsy of the vaginal vault was done on suspicion of a residual tumor, but histology testing showed no sign of this. A positron emission tomography (PET)–computed tomography scan showed 4 PET-positive areas in the lungs (Fig. 7). After this finding, the woman was referred to an oncologic department for initiation of chemotherapy. As of this writing, the patient is alive and still receiving chemo.

Positron emission tomography scan showing lung metastasis from leiomyosarcomas.
Discussion
The article presented a case of unsuspected LMS that was initially treated as a benign fibroid with UPA. Surprisingly, the LMS responded to this treatment in the same way as a benign fibroid and the patient's bleeding ceased. The presence of progesterone receptors in LMS has been documented, so perhaps this effect should have been expected. Attempts to treat LMS with aromatase inhibitors have been made, but only short-term disease control was measured and results were not entirely convincing.11,12 The concern is that, in this case, the UPA treatment actually led to a delay in the diagnosis with a larger or even metastatic tumor as a consequence.
A similar problem arises when treating leiomyomas with uterine artery embolization (UAE). Several cases with unsuspected LMS have been reported after UAE.13–15 and, as in the current case, delay of diagnosis was a main concern. There is an unsurprising pattern, wherein uncomplicated UAE leads to a delay of ∼6 months. UAE with complications (e.g., endometritis and vaginal shedding of necrotic tissue shortly after UAE) forces physicians to perform subacute hysterectomy, thus revealing any LMS.
The question is, of course, whether the LMS—in cases with prolonged effects of UAE or UPA—are able to generate metastases in this window between initiation of treatment (UAE or UPA) and surgery. UAE treatment does not appear to spread the disease in itself, 16 and this is not expected to be the case with UPA treatment either. In addition, in animal research, UPA has not been shown to be carcinogenic in itself. Doses 67 times human therapeutic exposure were given to rats without producing carcinogenic effects. 17 One could even imagine that both treatments could cause a temporary halt in the tumor development, given that UPA has been suspected to inhibit angiogenesis through the antagonistic effect on vascular epithelial growth factors. 18 In the histology testing of the current case, the tumor expressed partial positivity for progesterone receptors. Furthermore, there are suggestions of UPA inducing apoptosis in leiomyoma cells by inhibiting antiapoptotic proteins. 19 Evidence however, is not very strong and primarily based on in vitro studies.
Literature describing the time-span of development of LMS metastases would be highly relevant but very little literature exists on this topic. The most relevant article, by Tirumani et al., noted a median metastasis-free interval of 7 months. 20 This article reported on an experience in a tertiary-care clinic, and as the researchers themselves stated, this could have caused some selection bias because patients are often referred to them with advanced disease.
Quite a few researchers found that prognosis is worsened when specimens are morcellated, compared to en bloc removal of the tumors.5–7 These researchers, however, did not evaluate this risk when doing contained morcellation. Upon looking closer at these reports, only very few of these specimens were actually laparoscopically morcellated but, rather, were morcellated vaginally or through laparotomy, or via other routes. The current authors use contained power morcellation. The uterus is removed before being placed in a bag and morcellated. The current authors consider this method to be safe and have found it to be feasible. A closed system is used and only an accidental perforation could cause a theoretical spill of the specimen. As described by Seidman et al., the risk of morcellating an LMS is ∼0.09%. 3 With the use of contained morcellation in durable bags with good visual conditions, the current authors believe that the risk of abdominopelvic contamination is eliminated. If the bag were damaged during morcellation, it would collapse and visualization would be obscured.
With no noninvasive diagnostic tests readily available for this kind of sarcoma, many physicians are confronted with a difficult task—to determine if LMS is present. Treatment with UPA must be initiated with careful consideration and selection of patients. Any sign of abnormalities surfacing in the course of treatment—like in the current case, unexplained high levels of CRP and persistent dull pain—should be evaluated and examined carefully. Thorough, informed consent, including the small, but potentially serious, risk of delaying or overlooking an LMS, should be included in this information.
Conclusions
To the current authors' knowledge, this is the first reported case of unsuspected LMS inadvertently treated with UPA. Further studies on the effect of UPA on LMS would be of great interest. Clinics keeping databases of their hysterectomies and myomectomies should consider registering previous use of UPA in their patients. This would lay the groundwork for retrospective evaluations of the extent of delayed diagnostics of LMS and, it is hoped, help determine which women be can treated safely with UPA and which women for whom this treatment is not safe.
Footnotes
Author Disclosure Statement
No competing financial interests exist.