
Abstract
Abstract
Introduction
A
Medical diagnoses and/or hospitalization may be traumatic for some patients and could lead to post-traumatic stress disorder (PTSD). 6 In susceptible patients, this development of PTSD may manifest as catatonia. 7 This article presents a case of laparoscopic-proven PID in a virginal patient, likely resulting from postmenstrual vaginal douching. The patient's clinical course was complicated by a catatonic conversion reaction. The current authors were unable to find any other published case report of this kind of occurrence, despite a search of PubMed, Google Scholar, and Scopus.
Case
A 43-year-old gravida 0, virginal, African-American patient presented with abdominopelvic pain, menorrhagia, and fever. Her last menstrual period had begun 2 weeks prior to presentation, with continued bleeding on the day of her evaluation. She reported a history of monthly vaginal douching with an over-the-counter consumer product. Her recent douche use occurred a week after the start of her last cycle (1 week prior to presentation), when she assumed her cycle was completed.
Two days after douching, this patient's vaginal bleeding returned, accompanied by fever and abdominal pain. She presented to the emergency department when her pelvic pain became unbearable. Her past medical and surgical histories were noncontributory, and she was not currently taking any medications. She had no prior hospitalizations prior to this event. She did, however, have a history of anxiety but was not currently under treatment or counseling. She was employed and lived at home with her parents. As stated previously, she had no prior coital activity and denied any history of sexual abuse. Her temperature on arrival was 100.8°F (orally), and her other vital signs were within normal limits. A physical examination revealed a clinically ill, but stable patient. Scant white, nonpurulent vaginal discharge was noted on speculum examination. Her examination was remarkable for cervical motion tenderness, lower pelvic pain on palpation, and adnexal tenderness during a bimanual exam. Psoas and obturator examinations were negative. Although mild guarding was noted, there was no evidence of a surgical abdomen (it was nonrigid and without rebound).
Results
Laboratory assessment revealed leukocytosis at 22,000, and a hemoglobin level of 9.1 mg/dL. Endocervical and vaginal nucleic acid amplification swabs were negative for Trichomonas, Neisseria, Chlamydia, and bacterial vaginosis organisms. Initial blood cultures were negative. A computed tomography (CT) scan of the abdomen and pelvis revealed bilateral, fluid-filled tubal structures compatible with hydrosalpinges. Uterine, ovarian, bowel, and bladder images were normal. Findings from the CT scan correlated with transvaginal two-dimensional ultrasound images (Fig. 1). A diagnosis of PID was made clinically and intravenous antibiotics were begun in accordance to Centers for Disease Control and Prevention (CDC) guidelines. 8 On hospital day 12, despite antibiotic therapy, the patient's leukocytosis and febrile morbidity failed to improve. Therefore, diagnostic laparoscopy was performed. Operative findings revealed bilateral hydrosalpinges with loculated peritubal adhesions. Laparoscopic needle drainage of the hydrosalpinges revealed purulent fluid, which was sent for culture. Appendectomy was performed at this time to rule out concomitant pathology. The appendicial specimen revealed subacute appendicitis without evidence of perforation.
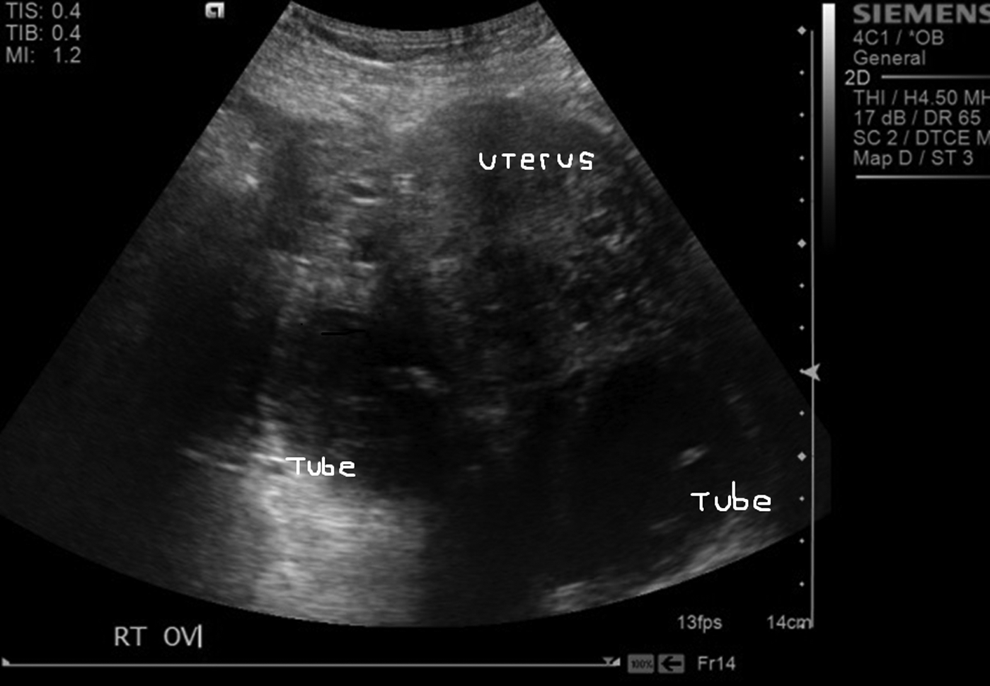
Transvaginal ultrasound of bilateral hydrosalpinges (257 × 178 mm).
An endometrial biopsy was also obtained intraoperatively; histologic review of the currettings was negative for architectural or stromal abnormalities. No histologic inflammation was found in the sample.
Culturing of the tubal aspirate revealed the presence of Escherichia coli as a single organism. Antibiotics were adjusted based on antimicrobial sensitivities of the aspirate. Clinical improvement followed, with normalization of her leukocytosis and temperature. However, despite this clinical resolution, the patient lapsed into a catatonic state. Via consultation with the neurology department, a brain CT/magnetic resonance imaging scan was obtained to look for organic etiology. This neuroimaging revealed no pathologic processes. Cerebrospinal fluid collected by lumbar puncture was negative for meningeal infection. A brain electroencephalogram showed normal brain activity, without evidence of epileptic activity.
Despite empirical trials of antipsychotic medications, antiseizure medications, and anxiolytics, this patient's mental state failed to improve. A multidisciplinary analysis of her condition—led by neurologists and psychiatrists—yielded the diagnosis of a catatonic conversion reaction. She was transferred to short-term inpatient rehabilitation with inpatient psychiatric evaluation. Although the patient's immediate family denied any past psychiatric diagnosis other than generalized anxiety disorder, the family concluded that her lack of coping mechanisms may have led to the development of this psychologic condition.
Discussion
The Centers for Disease Control and Prevention (CDC) has estimated that >1 million women experience an episode of PID every year, although the true prevalence may be higher because of undetected asymptomatic infection and/or misdiagnosis. 8 The condition leads to ∼2.5 million office visits and 125,000–150,000 hospitalizations yearly. 9 The organisms most commonly isolated in cases of acute PID are Neisseria gonorrhoeae and Chlamydia trachomatis. 10 However, cultures of specimens collected during laparoscopies have demonstrated that PID is a polymicrobial infection in as many as 30%–40% of cases. 11 The mechanisms by which microorganisms ascend from the lower to the upper genital tract is unclear. Although cervical mucus provides a functional barrier against upward spread, cervical dilation during menstruation, along with retrograde menstrual flow, may also facilitate the ascent of microorganisms. The practice of vaginal douching during or immediately after menstruation may facilitate upper-tract migration of vaginal flora further.
Vaginal douching is a common practice among women worldwide and is used for personal hygiene, religious traditions, and cultural reasons. 12 According to a cross-sectional observational study of 469 women practicing routine douching, the practice was significantly associated with a higher percentage of women having a history of PID (odds ratio [OR]: 2.4). 12 This association has been published by other sources as well. According to the PID Evaluation and Clinical Health (PEACH) study, researchers used logistic regression to adjust for background and other risk factors for PID (including a history of PID, having a new partner, smoking, and using cocaine) among 654 women ages 14–37, across 13 different national sites, who presented with symptoms of upper genital–tract infection. Women who had douched within 6 days prior to becoming symptomatic retained an elevated risk of upper genital–tract disease (OR: 1.7). 13
The current case study documents a history of recent douching as the only risk factor for PID in a virginal patient. The literature is scant with respect to PID in virginal patients. Cho et al. conducted a retrospective chart review of 122 patients diagnosed with PID via surgery; of these, 5 women were virgins (4.1%). In these 5 patients, no possible source of infection was identified, except in 1 who had a history of a previous appendectomy because she had a ruptured appendix with possible seeding of the fallopian tubes. 2
Regarding the current patient's conversion reaction, without prior documentation of a psychiatric condition, the default diagnosis was catatonic conversion reaction, possibly resulting from the emotional stress related to a first-time hospitalization and surgical intervention. In susceptible patients, this development of PTSD may manifest as catatonia. 7 However, the current authors acknowledge that labeling PID as the sole inciting factor for the conversion reaction may prematurely dismiss other preexisting, yet undiagnosed, psychiatric conditions. The patient is scheduled to continue to undergo psychologic evaluation and analysis.
The current authors' patient management scheme was in accordance to published guidelines for PID. 8 Despite intravenous antibiotics and consultation with specialists in infectious diseases, the patient did not improve with pharmaceutical therapy. This patient, thus, required laparoscopic surgical evaluation. Only after drainage of the purulent material did clinical improvement follow. As clinical treatment followed preexisting practice recommendations, it is the current authors' opinion that all other options were exhausted prior to surgical intervention.
Conclusions
Although most cases of PID are related to sexual activity, endogenous vaginal flora may lead to upper genital–tract infection. Douching may facilitate that process. E. coli is a known pathogen for the causation of PID 14 and was the bacterium identified in this case. Therefore, we agree with Cho et al., that “PID in virgin women is rare, but it should be considered in all women with abdominal pain, regardless of sexual history.” 2
Footnotes
Author Disclosure Statement
Hector Chapa is a medical consultant to Bayer Women's Healthcare and Medtronic, Inc. He has no relevant commercial disclosures pertaining to this report. No relevant commercial disclosures pertaining to this report exist for the other authors as well.