
Abstract
Abstract
Introduction
A
Case
A 43-year-old woman was referred to the outpatient university gynecology clinic of the Texas Tech University Health Sciences Center School of Medicine, Amarillo, TX. She had secondary dysmenorrhea and deep (collisional) dyspareunia following a GEA procedure performed 10 years before. She had also undergone laparoscopic tubal sterilization 4 years prior to the ablation procedure.
One year before her GEA, a LNG-IUS (Mirena,®; Bayer HealthCare Pharmaceuticals, Whipanny, NJ) was placed into her endometrial cavity without incident for anovulatory bleeding (AUB-O). The patient's medical records revealed that a transvaginal ultrasound was normal prior to the IUD placement. The LNG-IUS was deemed ineffective for bleeding control; thus, bipolar radiofrequency GEA (using a NovaSure,® radiofrequency generator; Hologic Inc., Marlbourough, MA) was performed with the LNG-IUS left in situ. The rationale for not removing the IUD could not be gleaned from this patient's medical record. IUD strings were visible on subsequent examinations. Following the GEA, the patient reported light monthly bleeding episodes but experienced new-onset dysmenorrhea and periodic deep dyspareunia. Ibuprofen was only marginally effective for controlling her dysmenorrhea.
In the presence of pelvic pain developing after GEA with the IUD in situ, an attempt was made to remove the IUD in an office setting, but the strings detached from the device suggesting embedding or perhaps uterine perforation. Transvaginal ultrasonography showed the IUD in the uterine cavity with limited extension into the myometrium.
Results
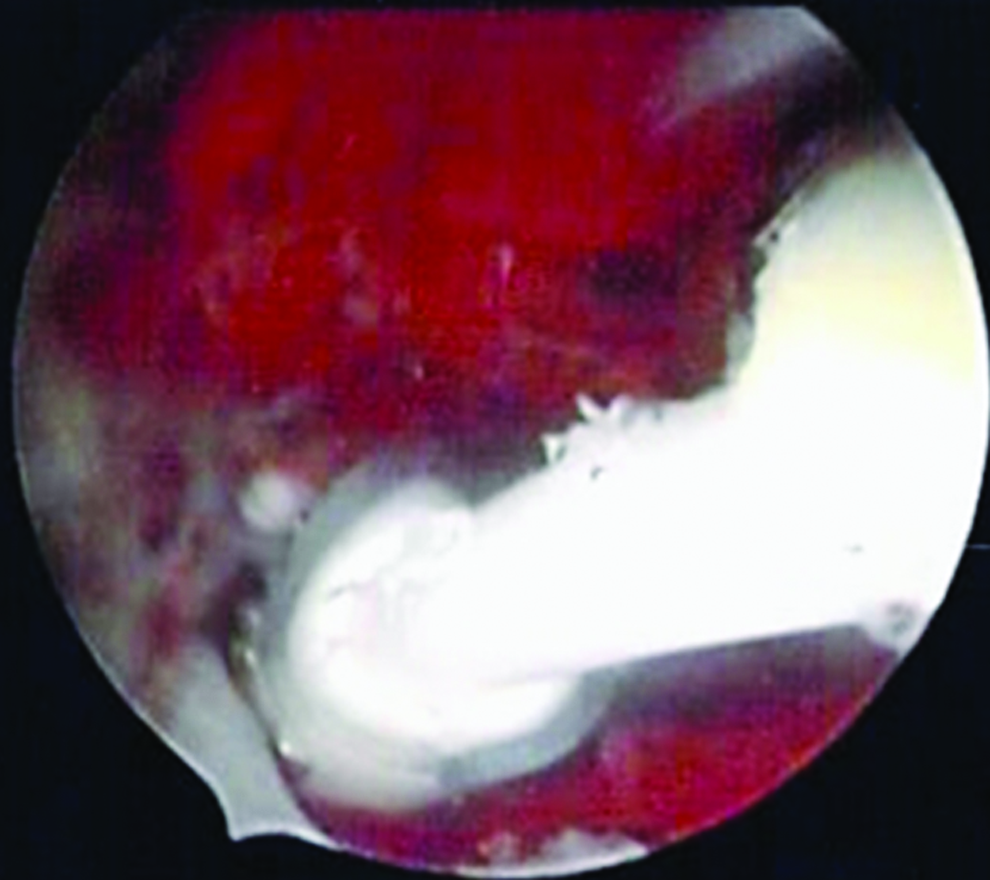
Operative hysteroscopy was performed in the operating room to remove the IUD incidental to a bilateral skin-sparing mastectomy for carcinoma of the breast. Hysteroscopy revealed 75% of the IUD device embedded in the myometrium below the scarred endometrial surface with only a small portion of the IUD shaft visualized (Fig. 1). An attempt to extract the device with a hysteroscopic grasper failed, and hysteroscopic scissors were used to dissect the upper shaft from the endometrial surface and myometrium (Fig. 2). The device was ultimately grasped and removed in one piece, and the plastic component was relatively intact architecturally despite thermodestructive effects associated with radiofrequency ablation (Fig. 3).

Hysteroscopic images of scarred endometrial cavity and only a small part of the levonorgestrel intrauterine system (LNG-IUS0 visualized superficially. Color images available online at www.liebertpub.com/gyn
Hysteroscopic image during dissection of the intrauterine device shaft from the scarred endometrium and superficial myometrium. Color images available online at www.liebertpub.com/gyn
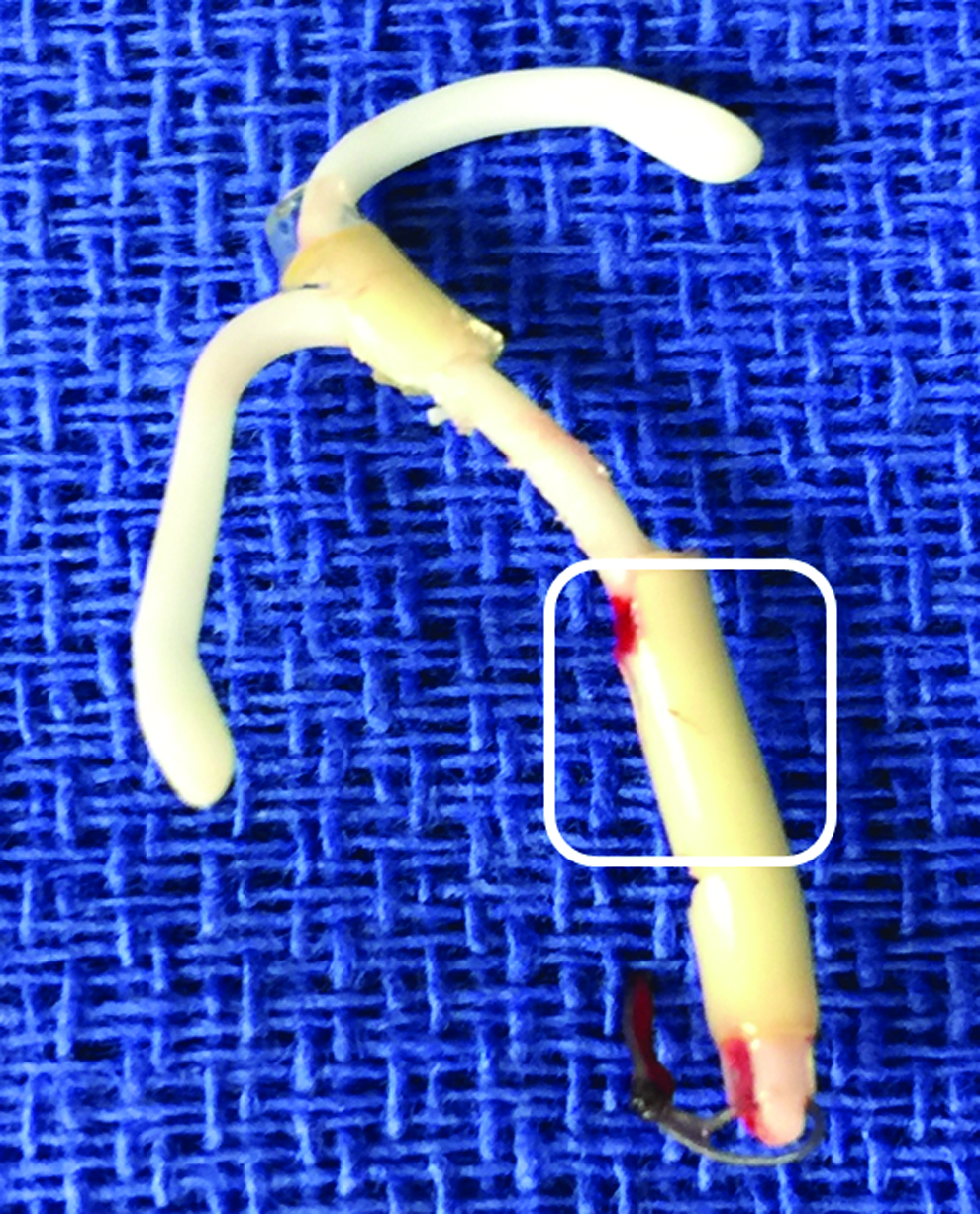
Postoperative image of the intact intrauterine device with the initially visualized portion of the shaft in the superimposed box. Color images available online at www.liebertpub.com/gyn
Postoperatively, this patient's pelvic pain was substantially reduced.
Discussion
The NovaSure radiofrequency generator delivers constant bipolar power up to 180 Watts with a power cutoff when tissue impedance reaches 50 ohms. The deepest destruction (5–7 mm) occurs at the mid-body of the uterus, where part of an IUD normally would be positioned. 3 In a review of the literature, no prior case reports were found regarding endometrial ablation performed with an IUD in utero. Not unexpectedly, the current patient's IUD had scarred into the myometrium making hysteroscopic removal challenging. Fortunately, the plastic component of the IUD did not disintegrate or melt under the higher tissue-level temperatures achieved during the radiofrequency GEA. Polyethylene, the plastic component of IUDs, softens at 80°C. and melts at 110°C–120°C. 4
In NovaSure's animal studies, performed prior to U.S. Food and Drug Administration approval, thermocouples placed 5–15 mm away from the radiofrequency external sheath recorded temperatures no higher than 10°C above body temperatures (corresponding to 47°C in the human). 5 It is noteworthy, however, that direct contact of the radiofrequency external sheath with a foreign body such as an IUD was not studied; hence, the precise temperature to which the IUD was exposed is unknown. In the case described, had plastic diffusion into the myometrium occurred, hysterectomy most likely would have been necessary to remove the IUD.
Given the onset of the symptoms and the improvement the patient had with surgical removal of the IUD, it appears that her dysmenorrhea and dyspareunia were likely caused by local inflammation and scarring associated with the embedded IUD. In the differential diagnosis, postablation tubal sterilization ablation syndrome 6 might also explain her dysmenorrhea and dyspareunia, but no evidence of synechia, hematometria, or hematosalpinx were noted at the time of hysteroscopy.
As noted above, this woman developed ER+, PR-, HER2- infiltrating ductal carcinoma of the breast. Data concerning removal of a LNG-IUS in the presence of breast cancer was discussed with the patient. Removal of the LNG-IUS is recommended under such circumstances despite little evidence to support the practice, and it remains uncertain whether the LNG-IUS increases the risk of breast-cancer recurrence.7,8
Conclusions
GEA is a viable treatment for premenopausal women who have chronic heavy menstrual bleeding and who desire permanent sterilization although endometrial ablation itself is not a sterilization procedure. Absolute contraindications to GEA include gynecologic malignancy, pregnancy, cervical or intrauterine infection, desire for future fertility, postmenopausal bleeding, and presence of an IUD. 1 IUDs should be removed prior to destructive ablation procedures although there is no practical or experimental data to support this recommendation.1,2 This case illustrates interesting physical and surgical findings when a plastic IUD was not removed prior to thermodestructive GEA and supports existing recommendations to remove IUDs before GEA.
Footnotes
Author Disclosure Statement
Each author declares no conflict of interest in the preparation of this article.