
Abstract
Abstract
Background:
Laparoscopic removal of a dermoid cyst carries a small risk of chemical peritonitis if intraoperative spillage of the cyst contents occurs. There are few reported cases of chemical peritonitis after iatrogenic intraperitoneal rupture of a dermoid cyst, and even fewer cases of prolonged chemical peritonitis.
Case:
A 35-year-old woman, G0, underwent laparoscopy for removal of a dermoid cyst. It could not be removed intact due to adhesions. The peritoneal cavity was irrigated before closure. Within days after surgery, the patient began experiencing fever, vomiting, and abdominal discomfort. A computed tomography (CT) scan showed peritonitis with ascites, right basilar pneumonia, and a right ovarian cyst with rim calcification. The patient was treated with intravenous and oral antibiotics. Over the next 2 months, her symptoms recurred, and she had two additional hospitalizations, thoracentesis, paracentesis, CT-guided percutaneous drainage and subsequent catheter repositioning, and two additional courses of antibiotics. Sixty-four days after surgery, she was reexplored laparoscopically to remove the calcified remnant. However, her symptoms persisted for another 2 months until she underwent laparotomy with incision, drainage, and debridement. She required drainage of fluid one last time and, since then, her symptoms resolved.
Results:
This patient had a 6-month course of complications related to chemical peritonitis from iatrogenic rupture of a dermoid cyst.
Conclusions:
Chemical peritonitis following intraoperative rupture of a cyst is a rare but potentially serious and intractable condition. Care should be taken to avoid intraoperative rupture. If rupture occurs, a thorough abdominal washout should be performed. If chemical peritonitis develops, early reoperation may be advantageous, especially if remnants are suspected. (J GYNECOL SURG 33:68)
Introduction
O
Dermoid cysts can be managed conservatively with ultrasound surveillance, or surgically, typically laparoscopically. Laparoscopic removal does incur a small risk of chemical peritonitis if intraoperative spillage of the contents occurs (0.2% incidence, Nezhat et al. 2 ). While rare, this aseptic inflammatory peritoneal reaction can have serious sequelae, including: abdominal-wall abscesses, adhesions, bowel obstruction, and fistulae. This article presents a case of a patient with chemical peritonitis after iatrogenic rupture, who, even after undergoing reoperation to remove residual cystic material, continued to have symptoms for several months.
Case
A 35 year-old woman, G0, initially presented for infertility evaluation and was found to have a 6.6-cm right dermoid cyst. She underwent laparoscopy during which the dermoid cyst could not be removed intact due to pelvic adhesions. A 2-cm calcified region of the dermoid cyst in the hilus of the ovary was left in situ due to its location and the preference not to perform oophorectomy, given the patient's desire for future fertility. The peritoneal cavity was copiously irrigated with 6 L of saline prior to closure.
This patient presented to the office on postoperative day #3 complaining of nausea, vomiting, fever, and abdominal discomfort. By postoperative day #7, after conservative management with antiemetics and nonsteroidal anti-inflammatories, without resolution of her symptoms, she presented to the emergency room. She was afebrile but had a white blood cell count of 26 K/UL and diffuse abdominal tenderness. A computed tomography (CT) scan showed peritonitis with ascites, right basilar pneumonia, and a right ovarian cyst with rim calcification (4.2 × 2.7 × 2.5cm). The patient was treated with intravenous (i.v.) antibiotics and was discharged to home on oral antibiotics after improvement in her symptoms.
Over the course of the next 2 months, the patient's symptoms were recurrent and she required two additional hospitalizations. She underwent thoracentesis and paracentesis for pleural effusions and perihepatic fluid collections, both of which were exudative, but cultures showed no growth. She subsequently had significant improvement in her symptoms, until her fever once again returned and a CT scan showed reaccumulation of her perihepatic fluid collection. She underwent CT-guided percutaneous drainage of the collection, wherein a catheter was left in place. One week later, the fluid collections had not resolved, and the catheter was changed and repositioned. She was treated with two courses of antibiotics during this time, but cultures continued to show no growth.
Based on the recurrent accumulation of ascites, the decision was made to reexplore laparoscopically and to remove the calcified remnant of the dermoid cyst. Thus, postoperative day #64 from her original surgery, this patient underwent a second laparoscopy. Numerous thin, filmy adhesions were noted in the abdomen (Fig. 1). A right cystectomy and a partial right oophorectomy were performed to remove the remnant (Fig. 2), and the pelvis was irrigated with 600 mL of normal saline. Despite this surgical intervention, this patient's symptoms persisted. Over the next 2 months, her perihepatic fluid accumulated once again, and, at first, was conservatively managed with antibiotics only but it continued to progress into multiloculated abscesses. The patient was eventually given an exploratory laparotomy with an incision, drainage, and debridement. Postoperatively, after a 2-day stay in the intensive care unit, a blood transfusion, i.v. antibiotics, and placement of a peripherally inserted central catheter (PICC) line, she was discharged to home on oral and i.v. antibiotics. Cultures again yielded no significant growth.
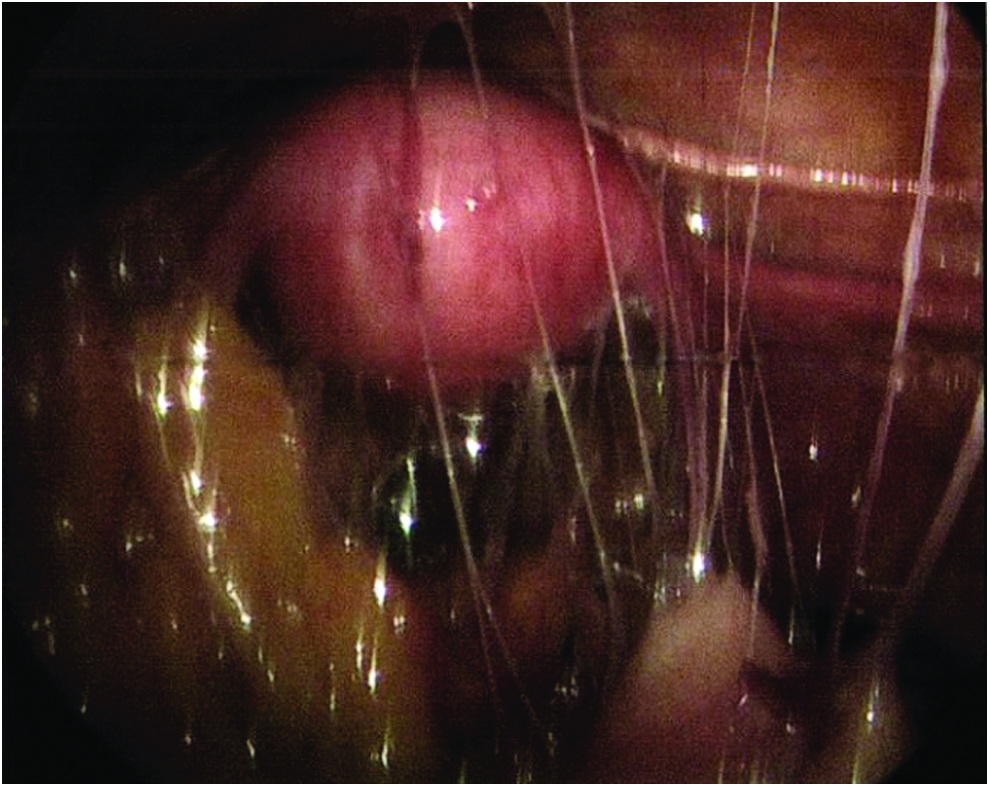
Numerous thin filmy adhesions seen upon entry into the abdomen during reoperation to remove the dermoid cyst remnant (230 × 183 mm).
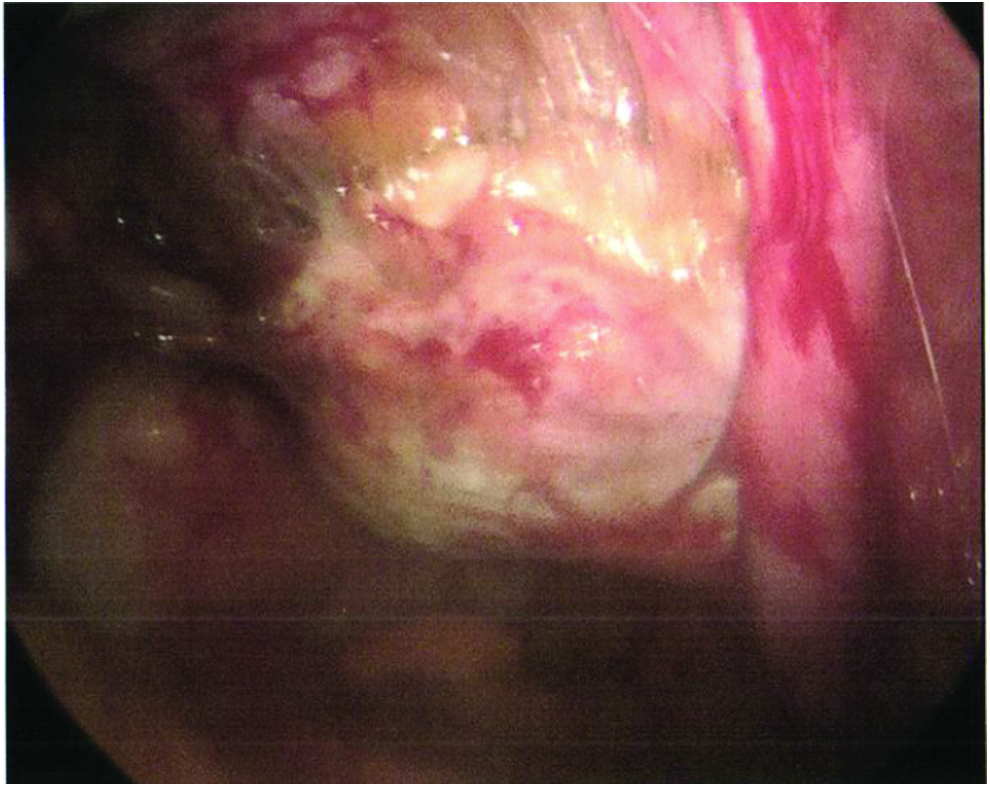
Right ovary/dermoid remnant as seen on reoperation (232 × 184 mm).
One week after discharge, a repeat CT scan showed new fluid collection. This was drained in the office by surgery.
The patient completed her courses of antibiotics, and her PICC line was removed. Her fluid accumulation and symptoms finally resolved, and she has since resumed her normal activities and is doing well.
Discussion
Chemical peritonitis following intraoperative spillage of dermoid contents is rare. Several studies on laparoscopic management of dermoid cysts have shown no cases of subsequent chemical peritonitis.2–6 There are few cases reported in the literature. One case showed rapid resolution of the peritonitis after removal of residual cyst contents and copious irrigation 3 days after the original procedure. 7 Malhotra et al. reported a case with a more complicated, protracted course. 8 Chemical peritonitis occurred 3 weeks after iatrogenic rupture of a dermoid cyst during a laparoscopic salpingo-oophorectomy. Reoperation, with the laparoscopy converted to a laparotomy for washout, was followed by enlarging peritoneal-fluid collections and development of an enterocutaneous fistula at the laparotomy wound. 8 Another case of prolonged chemical peritonitis, lasting 1 year, occurred when dermoid contents were left in the peritoneal cavity for over 2 weeks. 9 While this was a case of spontaneous rupture rather than an intraoperative rupture, it is interesting to consider the length of exposure of the peritoneum to the cyst contents when considering the outcome.
For the current patient, iatrogenic rupture of her dermoid cyst and spillage of its contents led to a 6-month course of complications related to chemical peritonitis, requiring multiple procedures, two additional surgeries, and several courses of antibiotics. The patient's reoperation, to remove a calcified remnant and to irrigate the area, occurred 2 months after her original surgery. Perhaps the prolonged nature of her peritonitis was related to the long exposure time of the peritoneum to the remaining portion of the dermoid cyst. This seems consistent with the few other cases in the literature. However, it may also be possible that the original spillage seeded the peritoneal cavity and continued to cause peritonitis despite removal of the remnant and copious irrigation. This might also have been possible in Malhotra's case, 8 in which there was no visible remnant at all.
Conclusions
Laparoscopic management of dermoid cysts has been shown to be safe and beneficial.2,10 However, it does incur a small risk of chemical peritonitis with intraperitoneal rupture, which has the potential to have an extensive course. Thus, this issue certainly warrants the attention of the gynecologic surgeon. Care should be taken to avoid intraoperative rupture and spillage; this care can be aided by the use of an endobag. If rupture occurs despite precautions, a thorough washout of the peritoneal cavity should be performed. In addition, all efforts should be made to resect the dermoid cyst completely. Should chemical peritonitis complicate the postoperative course despite these measures, there may be benefit to early reoperation, especially if remnants are suspected.
Footnotes
Author Disclosure Statement
None of the authors has anything to disclose.