
Abstract
Abstract
Introduction
S
Case
The patient was an 18-year-old gravida 3, para 1-0-1-1 female at 38 weeks' gestation, admitted for induction of labor for poorly controlled gestational diabetes. Her past obstetric history was significant for a previous cesarean delivery that was required to address arrest of dilation, and a pregnancy complicated by a fetus with an omphalocele; that pregnancy was terminated at 13 weeks. She reported having regular menstrual periods prior to the current pregnancy and had no other contributory history. There were no abnormal findings noted on a pelvic examination. She did not have facial acne or hirsutism. The patient underwent induction of labor with pitocin and a transcervical Foley balloon. Because of a category 2 tracing remote from delivery, she underwent a repeat cesarean delivery.
Upon inspection of the left adnexa at the time of the cesarean delivery, a large cystic and solid-appearing mass, measuring 12 × 14 cm, was noted extending from the left ovary. This was removed from its pedicle on the ovary. The other ovary was unremarkable in appearance. The male infant was normal in appearance with Apgar scores of 8/8.
Results
The specimen received was soft, but solid, and measured 12 × 10 × 7 cm. On the cut surface, the tumor was noted to be bright yellow and lobulated (Fig. 1). Histologically, it was composed of sheets of eosinophilic cells (Fig. 2) with areas of vacuolization (Fig. 3), consistent with lipid. There were up to 2 mitoses per 10 high-power fields. The tumor stained for calretinin, inhibin, and smooth-muscle actin, and was negative for cytokeratin 7 and desmin. The diagnosis was a steroid-cell tumor.

The tumor was bright yellow on a cut surface.
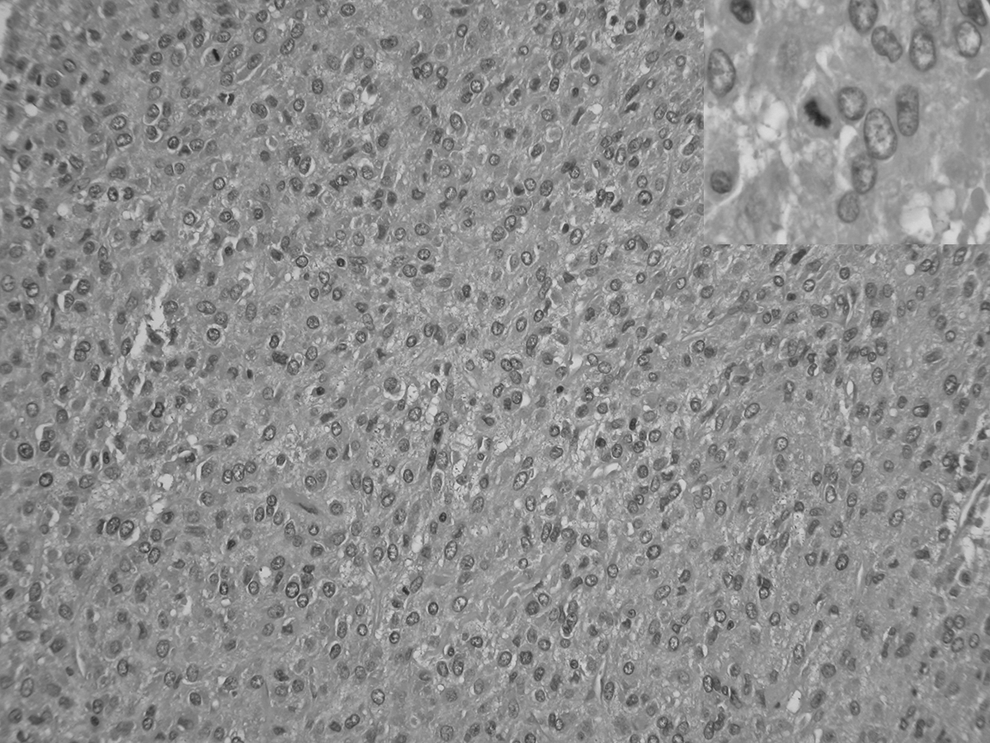
The tumor was composed of sheets of cells with abundant eosinophilic cytoplasm. Occasional mitoses were seen (inset), ∼2 per 10 high power-fields.
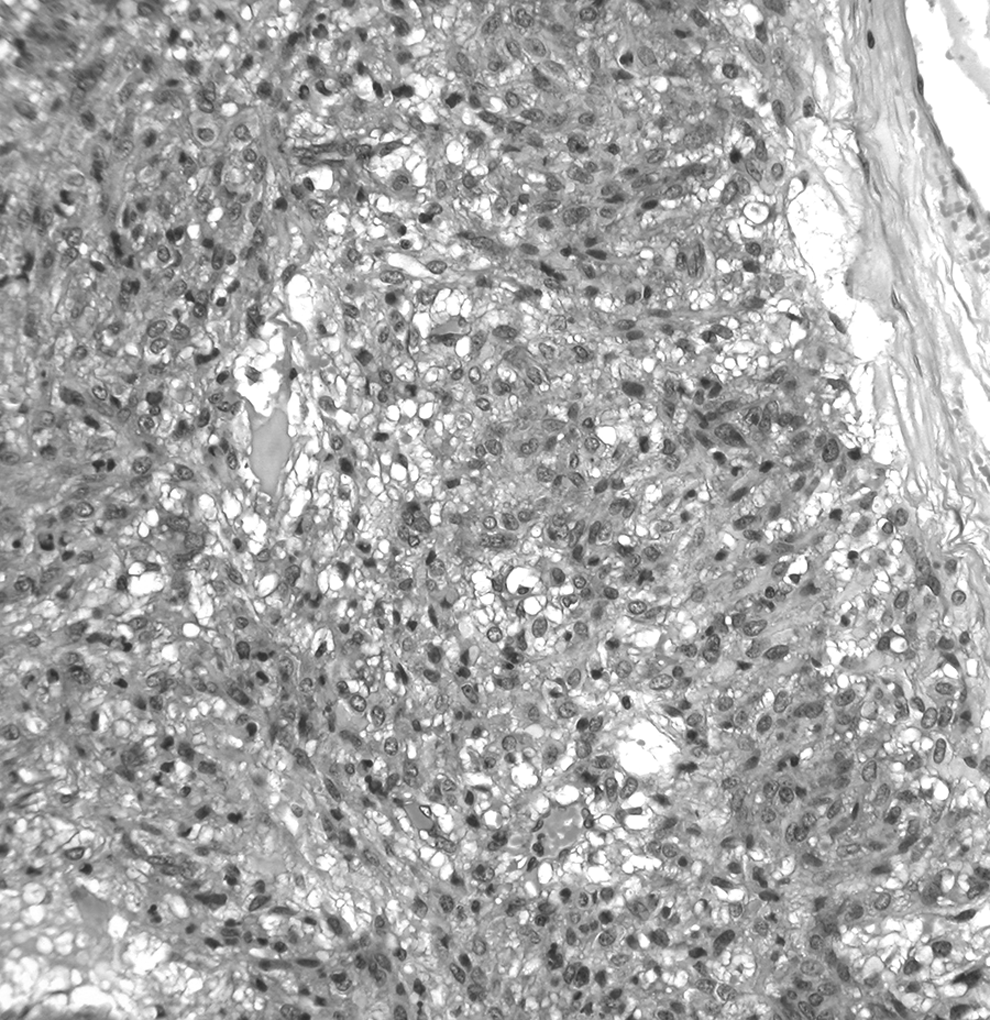
Multifocal areas showed vacuolization, consistent with lipid.
Discussion
Steroid-cell tumors of the ovary are rare, especially during pregnancy, with only a few reported cases. Steroid-cell tumors are classified into three subtypes: (1) steroid-cell tumor NOS; (2) stromal luteoma; and (3) Leydig-cell tumor. Steroid-cell tumor NOS is the most common, accounting for more than half of these tumors. These tumors usually have a greater age of onset, with an average age 43 at presentation, with no associations with pregnancy. 4
About 25% of these tumors have no hormonal manifestations, with patients experiencing no or vague symptoms, such as abdominal distension and pain. 5 The current patient fell into this category because she had an asymptomatic presentation with incidental discovery of the tumor during a cesarean section.
Steroid-cell tumors occurring in pregnancy can be difficult to distinguish from luteoma of pregnancy. Steroid-cell tumors are usually unilateral and yellow, compared to luteomas of pregnancy, which are most often bilateral and brown. 2 Steroid-cell tumors are often positive for fat stains corresponding to the vacuolated cytoplasm, as was seen in the current case, which helped favor that diagnosis.
Hayes and Scully found that 25%–43% of steroid-cell tumors are found to be malignant, and histologic examination can provide clues to predict malignant behavior accurately. 4 The researchers found that the most accurate predictor of malignant behavior was >2 mitotic figures per 10 high-power fields. Other features associated with malignant behavior are grade 2–3 atypia, necrosis, hemorrhage, and a diameter of >7 cm. 4 Tumor diameter >7 cm was associated with malignancy 78% of the time. The current patient's tumor was ∼12 cm with 2 mitoses per 10 high-power fields, indicative of a need for close follow-up.
There are no well-established protocols for treating this rare tumor. The primary mode of management is surgical excision, although chemotherapy has been utilized in some cases. The management of asymptomatic adnexal masses in pregnancy continues to be challenging, as management guidelines are mainly based on case-control or observational studies. 6
A review of the literature revealed two other cases of steroid-cell tumors which were associated with pregnancy.3,5 The first case was a 20-year-old female who had a full-term pregnancy 9 months after surgical intervention for a steroid-cell tumor NOS. 5 The second case was a 24-year-old female who was found to have an 8-cm, solid homogenous mass excised at delivery of a male fetus at 39 weeks by caesarean section. 3 Both cases presented with virulization of the mother.
Conclusions
In the current case, a steroid-cell tumor in pregnancy was detected incidentally during caesarean section. The occurrence of this lesion in pregnancy is exceedingly rare, and the lesion must be distinguished from luteoma of pregnancy, which is a hyperplastic rather than neoplastic condition.
Footnotes
Author Disclosure Statement
No competing financial conflicts exist.