
Abstract
Abstract
Introduction
A
Case
A 45-year-old premenopausal, multiparous woman presented with a complaint of pain in her lower abdomen for 1 week prior to her presenting. The pain was dull, aching, and mild. She also had a history of dysuria since 1 week. There was no history of any menstrual irregularity. A vaginal examination revealed the presence of a cystic mass that was felt in the posterior fornix and extending up to the suprapubic region. The patient's uterus was acutely anteverted and normal in size. There was no ascites. An ultrasound scan of her of pelvis showed a normal uterus with a cystic mass behind it. Computed tomography (CT) showed a multiloculated cystic lesion displacing the uterus anteriorly. The left ovary was normal but the right ovary could not be visualized. A diagnosis of an ovarian tumor was made. However, the patient's CA-125 level was normal.
This patient underwent an exploratory laparotomy. Intraoperatively, a retroperitoneal cystic mass measuring 20 × 15 cm was noted (Fig. 1). It had pushed the uterus anteriorly did not arise from it. Bilateral ovaries were normal. This retroperitoneal mass had a smooth surface (Fig. 2) but had burrowed deep to the level of the levator ani muscle. A hysterectomy had to be performed to facilitate complete excision of this mass.

Retroperitoneal cystic mass behind the uterus; both ovaries are normal.
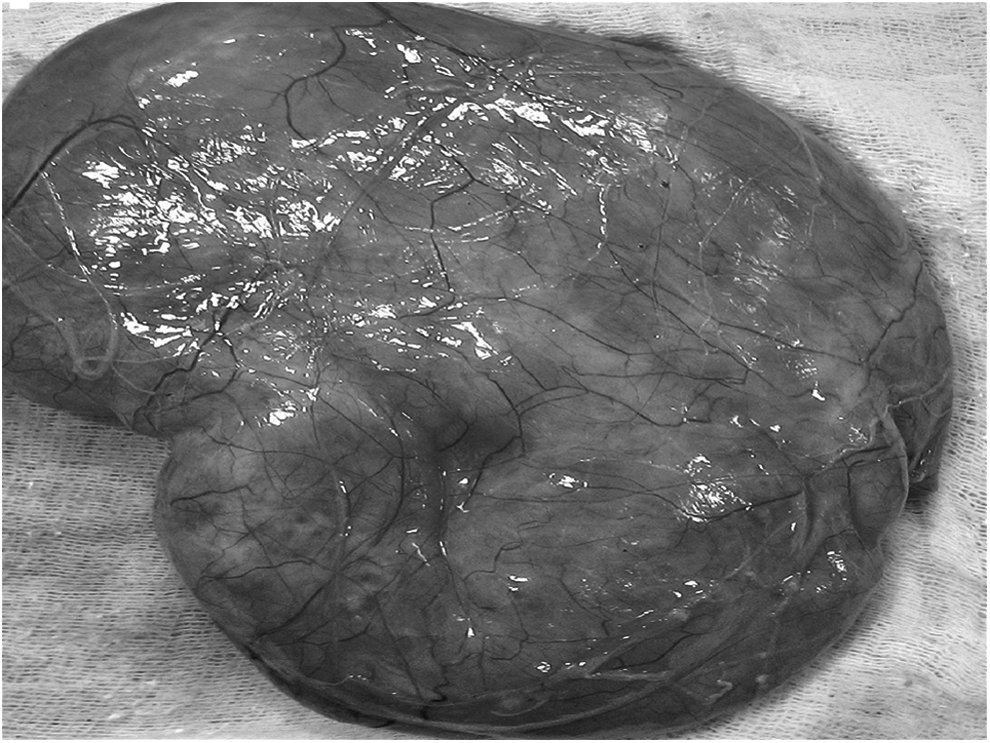
The excised retroperitoneal tumor with smooth surface and prominent blood vessels.
Results
The patient's postoperative course was uneventful.
Microscopically, tumor sections showed smooth-muscle bundles, adipocytes, and blood vessels (Fig. 3). There were no mitotic figures, epitheloid cells, or necrosis. Immunohistochemistry testing revealed that smooth-muscle actin and CD 34 were positive. Immunoreactivity was not seen with HMB[β-hydroxy β-methylbutyric acid]-45 and a diagnosis of an angiomyolipoma was made.
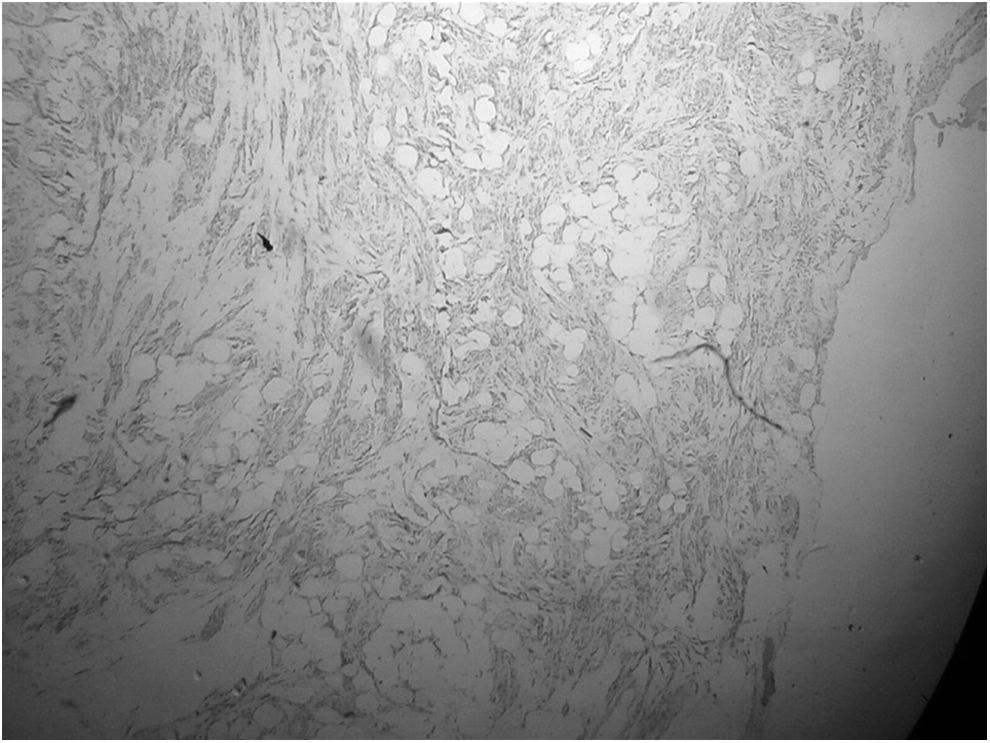
Tumor sections showed smooth-muscle bundles, adipocytes, and blood vessels.
The patient is currently undergoing regular follow-up.
Discussion
Retroperitoneal ERAML is a rare condition; < 20 cases have been reported as recently as 2012. 4 In each of these cases, the location of the tumor was either in the perinephric or peripancreatic space. One case of pelvic ERAML was reported in the preperitoneal space. 6 This current case is the first reported case of retroperitoneal ERAML arising in the pelvis.
Nearly 30%–40% patients with renal angiomyolipomas may have features of tuberous sclerosis. 7 However, this association is not commonly seen in cases of ERAML. 8 The current patient did not have any features of tuberous sclerosis.
The most common symptom in patients with retroperitoneal ERAML is nonspecific abdominal pain; this symptom occurred in the current patient. 4 Sometimes, patients with ERAML might present with shock caused by retroperitoneal hemorrhaging. 9 Less commonly, they can present with symptoms of ureteric obstruction or with an inguinal mass.10,11 The mean age of patients with retroperitoneal ERAML has been reported to be 45 years with a male-to female-ratio of 1:5.3. 4
Imaging studies, such as CT, may help with differentiating ERAML from other retroperitoneal masses, such as liposarcomas, lipomas, neurogenic tumors, lymphomas, and renal and adrenal tumors. Studies have shown that fat-dense lesions in CT and aneurysmal dilatation of the intratumor vessels seen on CT angiography suggest a diagnosis of angiomyolipoma. 12 There was an absence of fat densities on the CT scan in the current case. Furthermore, the presence of cystic changes in the lesion was unusual. Only 1 case of cystic degeneration in a uterine angiomyolipoma has been reported as of 2009. 5
Immunoreactivity to melanocytic markers, such as HMB-45, is characteristic of renal angiomyolipoma. 8 However, this immunoreactivity to HMB-45 might not be seen in all cases of ERAML.2,5 In the current patient, immunoreactivity to HMB-45 was absent.
Surgical excision is the primary modality of treatment; the objective is complete removal of the tumor and confirmation of the diagnosis. 10 Tumor embolization has also been used to manage this condition. 13
Very rarely, ERAML may recur or become malignant. The presence of an epitheloid variant and high mitotic activity might indicate the aggressive nature of such a tumor, increasing the risk of recurrence and metastasis. 14 Regular follow-up of these patients with CT imaging at regular intervals is necessary.
Conclusions
ERAML should be considered in the differential diagnosis of tumors arising from the pelvic retroperitoneum. Cystic degenerations might be seen in ERAML. HMB-45 staining may be negative in ERAML.
Footnotes
Author Disclosure Statement
No competing financial interests exist.