
Abstract
Abstract
Introduction
C
Conventionally, cornual pregnancy is treated via laparotomy with cornual resection or hysterectomy. However, with the introduction of laparoscopic surgery, there are abundant reports on laparoscopic cornual resection, salpingostomy, or cornuostomy whenever possible, even in emergent rupture cases.2,3,5–40
Because of the technical challenges and requirements for laparoscopic suturing, there are conflicting data3,23–40 regarding whether or not conversion to laparotomy still occurs in surgical treatment for cornual pregnancy. For example, Tinelli et al. 5 treated 3 patients laparoscopically by salpingotomy or resection of the cornual region of the uterus and suturing of the incision site with no need for conversion; yet, a rate of 9% for conversion to laparotomy was reported in a small case series of 11 patients. 6
In contrast to cornual ectopic pregnancy, tubal ectopic pregnancy is treated mainly by laparoscopy, and in the pursuit of better cosmetic outcomes and less morbidity, single-incision laparoscopic surgery (SILS) was developed in recent years. 7 Procedures, such as adnexectomy, hysterectomy, myomectomy, ovarian cystectomy, and salpingostomy can now be treated using this approach.41–47 These studies have reported a good safety profile for—and the feasibility of—SILS with potential reduction in postoperative pain, wound infections, and entry complications.
Therefore, SILS is rapidly gaining popularity for laparoscopy for tubal ectopic pregnancy, but to the current authors' knowledge, reports on using SILS for cornual ectopic pregnancy are extremely sparse; there were only two reports48,49 with a total of 3 cases reporting the successful use of SILS for addressing cornual ectopic pregnancy.
One reason for the relative lack of use of SILS for cornual ectopic pregnancy is potential torrential bleeding. 2 A large amount of hemoperitoneum, which obscures vision and the need for laparoscopic suturing, renders laparoscopic treatment of cornual ectopic pregnancy unpopular. SILS is also technically more challenging than conventional laparoscopy, as 2–3 instruments have to go through one single umbilical incision. The resultant crowding of the instruments and in-line viewing with external clashing of instruments 43 might also explain why few surgeons attempt this approach for laparoscopic treatment of cornual pregnancy.
A randomized prospective trial 50 showed that the ENDOLOOP® ligature is an equally effective and safe alternative to electrocautery for laparoscopic salpingectomy for patients with tubal ectopic pregnancies, and the ENDOLOOP ligature has been used for in laparoscopic surgery for cornual ectopic pregnancy. 40 For the current case, this article describes a simplified SILS approach for treating a right cornual ectopic pregnancy, using two ENDOLOOP ligatures to secure hemostasis and facilitate excision of the cornual ectopic pregnancy. With this technique, surgeons may find it easier to adopt the SILS approach for treating ectopic pregnancies. It is hoped that surgeons would consider this method for future suitable patients presenting with cornual ectopic pregnancies.
Case
Case summary
The patient was a 27-year-old Chinese female who presented at the National University Hospital, in Singapore, with right iliac fossa pain. She reported a history of irregular menstruation and no previous medical or surgical history of note. Her serum β-human chorionic gonadotropin (β-hCG) level was 16,673 IU/L, and a bedside transvaginal ultrasound test showed a 19-mm gestational sac with a yolk sac and fetus (crown–rump length = 14 mm) in the right adnexae (Fig. 1). No fetal heart activity was seen, and minimal fluid was visible in the pouch of Douglas. She remained stable with a preoperative hemoglobin level of 13.6 g/dL.

Transvaginal ultrasound of pelvis showing 19-mm gestational sac with presence of a yolk sac and fetus (crown–rump length = 14 mm) in the right adnexae.
Operative procedure
An emergency diagnostic laparoscopy was arranged. As this patient was hemodynamically stable, she was offered the SILS approach, which she accepted. She was placed in a lithotomy position and surgery was performed under general anesthesia. A 1.5-cm transumbilical incision was made and Karl Storz X-cone Device® was inserted into the peritoneal cavity via open Hasson's entry method (Fig. 2).

Karl Storz X-cone Device® inserted into the peritoneal cavity via open Hasson's entry method with single bent laparoscopic instrument and scissors.
Intraoperatively, a 3-cm, right-cornual ectopic pregnancy was visualized. Minimal hemoperitoneum of 50 mL was seen. Vasopressin, in a dose of 10 U in 20 mL of normal saline, was injected into the base of the ectopic pregnancy. The first ENDOLOOP was tightened around the base of the ectopic pregnancy. Caution was taken to avoid over-tightening the loop as the suture could have cut into the uterine wall, causing further bleeding. A second ENDOLOOP was then placed above the first loop. Partial extrusion of the ectopic pregnancy occurred when the second loop was tightened. The cornua of the uterus that contained the ectopic pregnancy were then excised, using a prebent laparoscopic grasper (Clickline Alligator grasping forceps; Karl Storz) and straight scissors with monopolar diathermy. Additional care was taken to ensure hemostasis over the excised site with bipolar diathermy. Minimal bleeding occurred during the procedure, as adequate hemostasis was attained with the two ENDOLOOP ligatures. The remainder of the fallopian tube was then excised easily (Fig. 3). The specimen was retrieved via the umbilical incision. The single umbilical incision was closed with Vicryl® sutures.
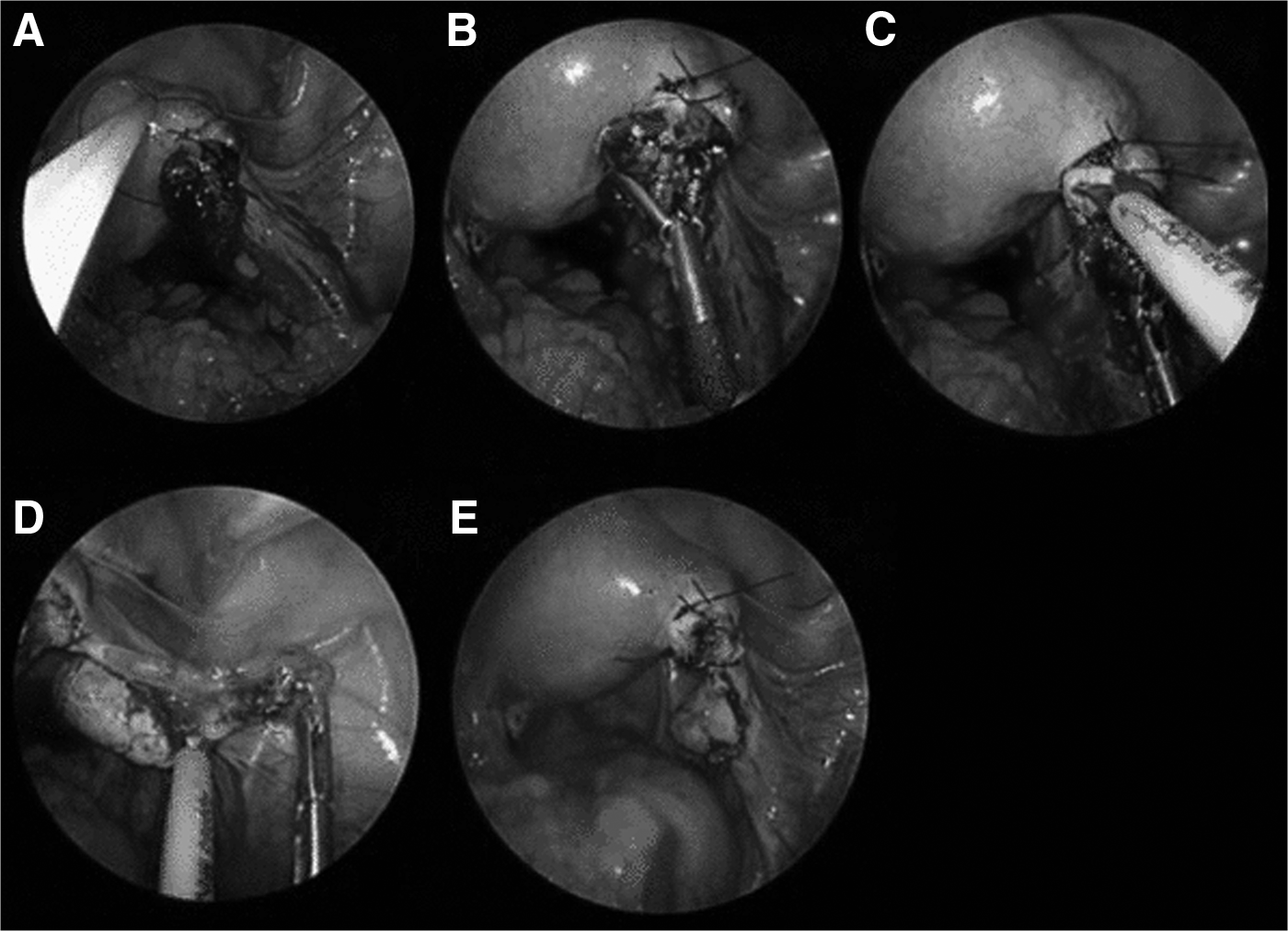
Single-incision laparoscopic surgery approach for resection of cornual ectopic using and ENDOLOOP®
Results
The cornual ectopic pregnancy was removed successfully, using the surgical technique described above. No conversion to conventional laparoscopy or laparotomy was needed. No perioperative surgical complications occurred. Operating time was 67 minutes. The patient recovered well postoperatively and serial β-hCG testing showed rapid resolution of the ectopic pregnancy.
Discussion
SILS is an attractive alternative to conventional laparoscopy because of SILS' superior cosmetic outcome.41–47 This advantage is especially important to young women who are likely to be interested in good cosmetic outcomes and reduced morbidities from less use of ports. The use of a single incision also reduces parietal-wall trauma and eliminates the risk of injuring the epigastric artery and bladder secondary to placement of the lateral and suprapubic trocars.
However, SILS remains a challenging technique, as 2–3 instruments are placed through a single small umbilical incision. Crowding, external clashing, in-line viewing, and limited working space 43 are the reported drawbacks of this approach. Nevertheless, recent studies have concluded that the feasibility and safety of SILS are equivalent to conventional laparoscopy. With advancements in technology and experience in SILS, operating time is likely to decrease over the years.
Cornual ectopic pregnancy has conventionally been a difficult variant to treat surgically.2,3,5–40 The risk of rupture with torrential bleeding is a major concern.2,3 In the last decade, the laparoscopic approach is gradually becoming the standard treatment for ectopic pregnancy. SILS could be utilized increasingly as surgeons attempt to push the boundaries of laparoscopic surgery.
In a case reported by Lee et al., 48 cornual resection was performed and extensive suturing of the defect was required to control the bleeding and secure hemostasis. SILS suturing is difficult, especially if performed in an emergency setting. Prolonged operating time or conversion to standard laparoscopy or even laparotomy is often the eventual outcome.
Therefore, the current authors propose using two ENDOLOOP ligatures to simplify the SILS approach for cornual resection and to achieve better control of hemostasis without the need for suturing. In this current case, after injecting vasopressin at the base of the cornual ectopic pregnancy, use of the first ENDOLOOP stopped the bleeding rapidly. This method provided time to aspirate the hemoperitoneum and improve visibility of the operating field, therefore facilitating proper intraperitoneal surveillance.
The second ENDOLOOP helped tighten the bleeding point with partial extrusion of the ectopic pregnancy. This second ENDOLOOP also minimized the amount of excision required and minimized damage to the uterine wall. Excision of the cornual ectopic pregnancy was achieved easily with a single prebent laparoscopic grasper and scissors using monopolar energy. Additional hemostasis was secured with bipolar diathermy. No suturing was needed.
A similar technique can be utilized in both conventional laparoscopy and SILS. As one gains experience in SILS, applying the ENDOLOOP technique to treat cornual ectopic pregnancies will become increasingly feasible and easy.
To the current authors' knowledge, this article is the first clinical report on the use of ENDOLOOP ligatures to facilitate surgical management with a SILS approach for cornual ectopic pregnancy. Larger clinical studies using this approach will ascertain the feasibility and advantages of this technique further.
Conclusions
Innovation often helps to optimize and improve surgical procedures, therefore leading to potentially higher patient satisfaction and outcomes. Although SILS is a challenging technique, use of ENDOLOOP ligatures can be applied safely and efficiently for SILS surgical treatment of cornual ectopic pregnancies. Patients who present with cornual ectopic pregnancies should be offered SILS if they are deemed suitable, as SILS has better outcomes in terms of improved cosmesis, and potential reduction in postoperative pain and wound infections. With this technique, surgeons may find the SILS approach less difficult to perform for treating cornual ectopic pregnancies, and, it is hoped, consider this method for suitable patients in the future.
Footnotes
Author Disclosure Statement
Neither author has any conflict of interest to report.