
Abstract
Abstract
Background:
Squamous carcinoma-in-situ (CIS) within a benign cystic teratoma is exceptionally rare, particularly in the absence of an adjacent invasive squamous component. Most of the few reported cases of CIS without invasive carcinomas occur in postmenopausal women and are usually incidental histopathologic findings.
Case:
A 35-year-old, gravida 1, para 1001, woman underwent exploratory laparotomy and bilateral ovarian cystectomies for bilateral ovarian dermoid cysts. They were excised and, via histopathology, were confirmed to be benign cystic teratomas. Six months later, the patient had pelvic pain and had a 7-cm left adnexal cyst. She underwent laparoscopic oophorectomy. The final diagnosis was invasive squamous-cell carcinoma of the ovary. A re-review of the slides of the bilateral cystectomies showed a minute focus of CIS in the right ovary that was opposite to the newer invasive carcinoma. p16 immunostaining was negative.
Results:
There was no evidence of malignancy or dysplasia in the sections of cyst taken from the left ovary during the original excision.
Conclusions:
In the absence of invasion, excision of the ovary with CIS appears to be adequate therapy. If CIS is detected histopathologically, a search for invasive elements should be undertaken. (J GYNECOL SURG 33:34)
Introduction
M
Case
Institutional review board approval was not required for this case report.
A 35-year-old, gravida 1, para 1001, woman underwent exploratory laparotomy and bilateral ovarian cystectomies for bilateral ovarian dermoid cysts. A 13 × 12 cm right and a 15 × 13 cm left cyst were excised and, via histopathology, were confirmed to be benign cystic teratomas. Six months later, the patient presented with pelvic pain and was found to have a 7-cm left adnexal cyst. She underwent laparoscopic oophorectomy for what was thought to be a recurrent dermoid cyst. The final diagnosis was invasive squamous-cell carcinoma of the ovary. A re-review of the slides taken from the bilateral cystectomies showed a minute focus of CIS in the right ovary (Fig. 1), which was opposite to the current invasive carcinoma. p16 immunostaining was negative.
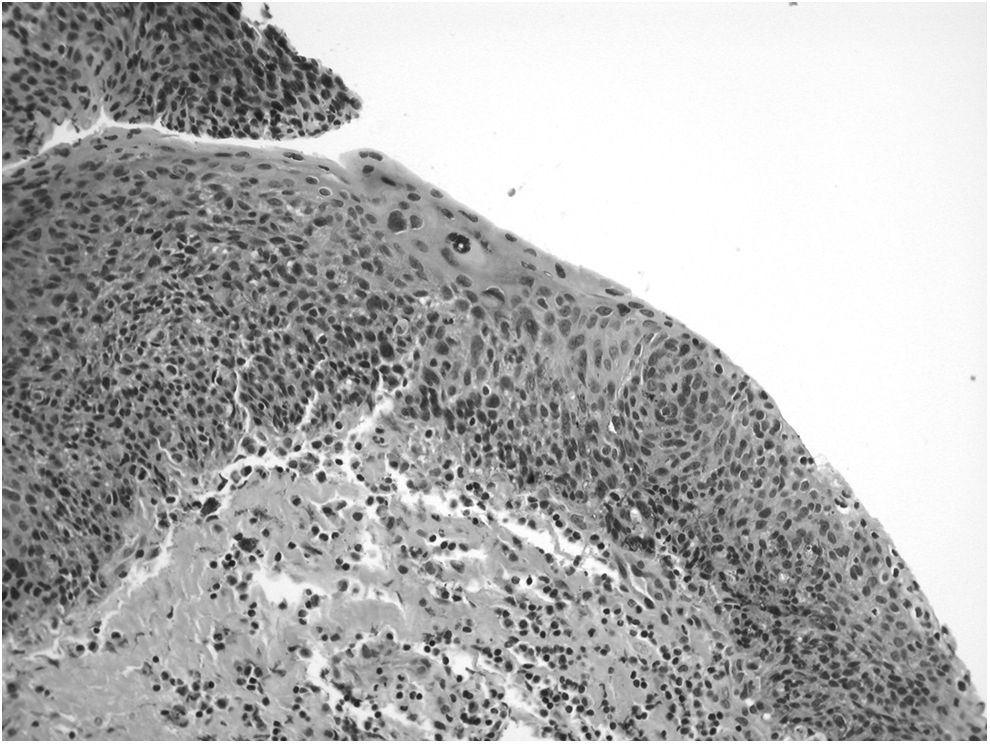
Carcinoma in situ within a teratoma.
Results
There was no evidence of malignancy or dysplasia in the sections of cyst from the left ovary at the original excision.
Discussion
Malignant degeneration in a benign cystic teratoma is estimated to occur in <2% of cases, and the majority of malignancies are squamous-cell carcinomas. 2 Squamous CIS in a dermoid cyst is exceptionally rare, particularly in the absence of an adjacent invasive carcinoma. A transition from CIS to invasion has been described in some cases,2–4 with 2 of 15 invasive squamous-cell carcinomas showing an in situ component in one series, 4 but only a few cases of CIS without invasive squamous-cell carcinoma have been reported (Table 1).5–12 CIS as the precursor lesion was supported further by the report of a case of “microinvasive” squamous-cell carcinoma arising in the ovary. 13 Because of the rarity of the finding, it is unclear what the expected behavior of CIS in a dermoid cyst would be; however, in a literature review of squamous-cell carcinomas in dermoid cysts, Chen et al. 14 found 5 cases of CIS in dermoid cysts, with 100% 5-year survival. While these researchers did not specify which cases these were, there was sufficient overlap in the researchers' reference list with the cases reviewed in the current article to conclude that most if not all were the same cases.
CIS, carcinoma-in-situ; TAH, total abdominal hysterectomy; LSO, left salpingo-oophorectomy; N/A, not available; BSO; bilateral salpingo-oophorectomy; RSO, right salpingo-oophorectomy; GI, gastrointestinal, NED, no evidence of disease, mo, month(s);
The limitation in the current case was the retrospective nature of the identification of the dysplastic focus in the original surgical specimen. Hence, it was only possible to claim that there was no dysplasia in the ipsilateral ovary based on the existing sections. Yet, it is reasonable to speculate that whatever molecular alteration caused the CIS in the contralateral ovary could have also had a similar effect on the ovary that developed the invasive carcinoma. It has been suggested that human papillomavirus (HPV) might play a role in the development of squamous neoplasms in dermoid cysts 15 ; however, p16 immunostaining, a surrogate marker of high-risk HPV, was negative in the current case as well as that of Gurrera et al. 11
The origin of CIS in the ovary is unclear. A case of an ovarian CIS arising 8 years after a radical hysterectomy for superficially invasive cervical squamous-cell carcinoma is of interest. In this case, there were no teratomatous elements in the ovary. 16 It is unlikely that the superficially invasive cervical tumor metastasized 8 years later, but the association of squamous neoplasia of the cervix and concomitantly in the ovary has been reported, and it has been suggested as being a field effect. 16 What lends some credence to this is the finding of HPV in some squamous-cell carcinomas of the ovaries. 15 In 1 case, CIS in the absence of a teratoma or other neoplasia was described. 17 While a frankly invasive squamous-cell carcinoma can arise in the ovary de novo, the researchers were unable to explain the origins of their case.
Although the majority of ovarian squamous-cell carcinomas arise in conjunction with teratomas, association has also occurred with Brenner tumors and endometriosis, and the associated elements should be sought.1,16 CIS within a dermoid cyst has been suggested to arise in squamous metaplasia arising from the columnar epithelium within the dermoid cyst, 1 much like the transformation zone of the cervix. The current case of invasive squamous-cell carcinoma found during the second procedure did not, at that time, show teratomatous elements. However these elements were present in the previous cystectomy specimen. Hence, it is likely that the carcinoma grew over any residual identifiable teratomatous elements.
It has been emphasized that findings suggestive of frank malignancy arising in a benign cystic teratoma include postmenopausal age, adhesions from the neoplasm, solid areas or areas of unusual thickness of the wall, and necrosis. 5 However, there are no specific preoperative findings indicative of CIS. It has been suggested that the infrequency of reported CIS in dermoid cysts is the result of potentially small microscopic foci. As in the current case, these foci, are not detectable grossly 11 and might not be detected on routine representative sampling of a dermoid cyst. 6 Cytologic examination may miss a malignancy, 12 and, in the current case, ovarian cyst fluid submitted during the first procedure only showed keratinaceous debris.
Conclusions
CIS arising in a dermoid cyst could be a precursor lesion of invasive squamous-cell carcinoma arising from dermoid cyst. Most reported cases were seen in postmenopausal women (Table 1). In isolated CIS, ovarian excision appears to be an adequate therapy. If CIS is detected, extensive sampling is warranted. Given the rarity of CIS in dermoid cysts, there is no reason to alter existing recommendations for observation of smaller presumptive dermoid cysts detected on ultrasound scans. There are not enough data to establish a definitive recommendation for performing ipsilateral oophorectomy for CIS discovered during a cystectomy. The approach to these cases should be individualized. Additional cases will add to the understanding of this rare lesion.
Footnotes
Author Disclosure Statement
No financial conflicts exist.