
Abstract
Abstract
Objective:
The goal of this research was to determine the efficacy and safety of laparoscopic treatment of vesicovaginal fistula (VVF).
Materials and Methods:
This was a descriptive, retrospective study of 36 patients with VVF who were treated between 2006 and 2015. This study included patients age 18 or older, with supratrigonal VVF caused by obstetric or surgical injuries, even when they had other lesions of the urinary tract. Patients with VVF located at the trigonal or pretrigonal levels, and who had prior pelvic radiotherapy or contraindications for the laparoscopic approach were excluded. A transperitoneal transvesical approach was utilized, with vesical and vaginal closure in a single layer, with running 2-0 Vicryl suturing, without interposition of other tissues. SPSS version 21 was used for statistical analysis of the data. Measures of central tendency dispersion, absolute frequencies, and percentages were used. The relationship between the intraoperative variables and the recurrent risk of fistula was analyzed. Student's t-test and Fisher's exact test were utilized; p < 0.05 was considered significant.
Results:
The average age was 46.5 years, 94.4% of VVF cases were due to open abdominal hysterectomy. The mean time interval between the appearance of the fistula and surgery was 14.7 months. Average operative time was 140.4 minutes. Average hospital stay was 7.8 days. No conversions to open surgery were required. The surgery was successful in 33 of 36 patients (91.6%). There were 3 complications (11.1%). The Dindo classification was Grade IIIb.
Conclusions:
Repair of VVF with laparoscopic surgery is an effective and safe procedure with a high success rate and is an alternative for treating VVF. (J GYNECOL SURG 33:175)
Introduction
V
Although a spontaneous closure of VVF with conservative treatment, with little efficacy, has been reported, in most patients, surgical treatment is essential for its repair. Several techniques to repair VVF have been described. The O'Connor technique is considered the “gold standard” for the treatment by the abdominal approach with a high success rate (85%–100%), and the Laztko technique is the treatment of choice for the vaginal approach.3–5
Following the principles of the O'Connor technique, laparoscopy has been more widely used in recent years with satisfactory perioperative results, acceptable success, and safety rates.6,7
The aim of this study was to determine the efficacy and safety of the laparoscopic approach for VVF.
Materials and Methods
The laparoscopic transvesical approach was utilized in 36 patients with primary or recurrent VVF between 2006 and 2015, in only one institution (the National Center for Minimally Invasive Surgery, La Habana, Cuba). A descriptive and retrospective study was carried out. Supratrigonal VVF caused by obstetric or surgical injuries were included, even when patients had other lesions of the urinary tract; trigonal or pretrigonal VVF patients with prior pelvic radiotherapy or contraindications for laparoscopic approach were excluded.
All patients underwent gynecologic examination, abdominal ultrasound, and intravenous pyelogram or UroTAC (CT scan with contrast of urinary tract) and cystourethroscopy. Antibiotic treatment with cephazolin and/or gentamicin was used when inducing anesthesia. The surgical technique began with cystoscopy for the placement of ureteral catheters and a 20-ch urethral Foley catheter.
Pneumoperitoneum was created with a Veress needle. Three trocars were placed: 10 mm (umbilical); 10 mm (right iliac fossa or on the side of the predominant hand of the surgeon); and 5 mm (left iliac fossa). In some cases, a fourth 5-mm suprapubic trocar was required. After filling the bladder with normal saline, a minimal incision was made in the bladder until the fistulous tract was identified and removed with scissors (Fig. 1) and submitted for pathologic evaluation. The plane between the bladder and the vagina was dissected and both were closed in a single layer with a running 2-0 Vicryl suture (Fig. 2). Saline solution was instilled through a Foley catheter to confirm that there was a watertight closure of the closed bladder defect, and a peritoneal drainage tube (a Nelaton catheter) was placed into the Douglas cul-de-sac. Ureteral catheters remained postoperatively in the patients for at least 3 days, and the Foley catheter was kept in place for 3 weeks. Biopsies of the fistula orifices were performed to obtain specimens from all patients and submitted for pathologic evaluation. All cases were operated on by the same surgeon (T.G.L.), at the National Center for Minimally Invasive Surgery.
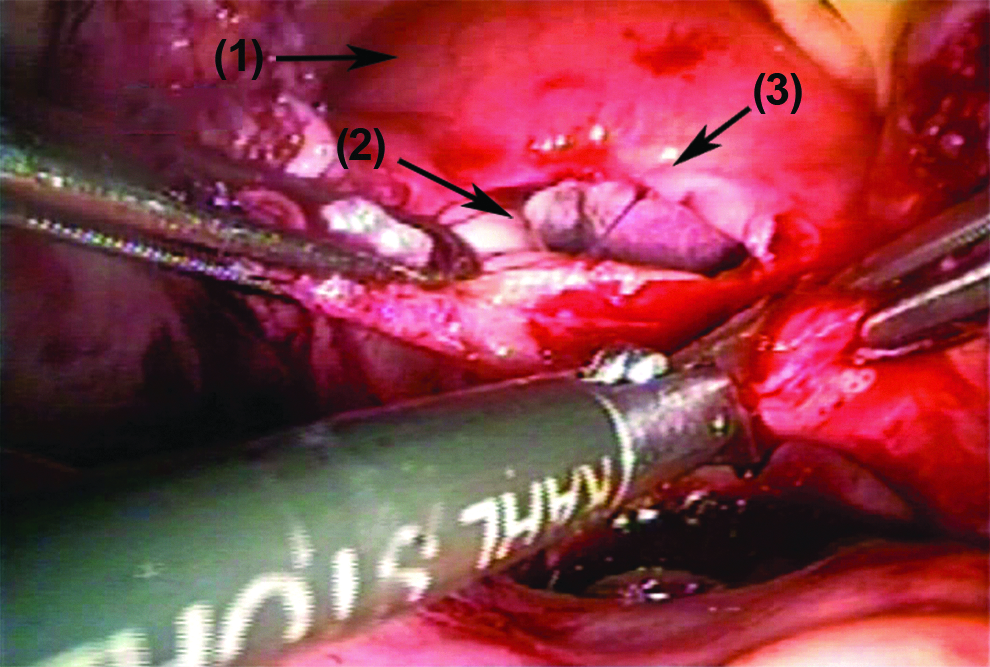
Fistulous tract resection:
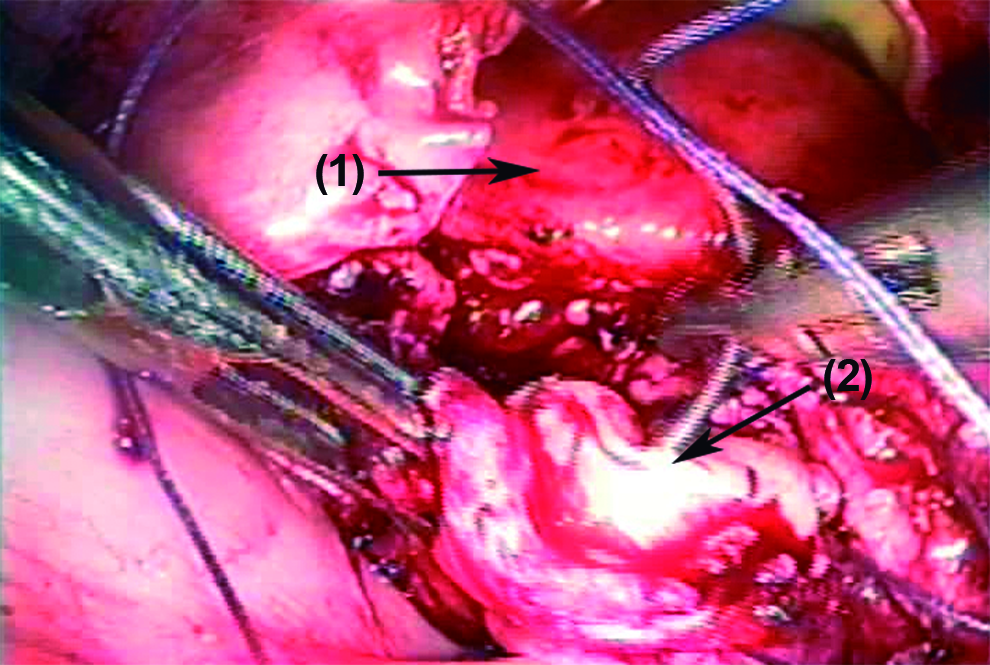
Single layer running suture of vagina:
Various characteristics of the patients (Table 1) were recorded along with the perioperative results (Table 2). Ethical aspects of the study were approved by an institutional ethical committee.
ASA, American Society of Anesthesiologists; SD, standard deviation; CI, confidence interval.
Patients with associated simultaneous surgical procedures were excluded in the calculation.
CI, confidence interval; SD, standard deviation; OT, operative time; URS, ureteric stone treatment.
SPSS, version 21, was utilized for statistical analysis. Measures of central tendency (average) and dispersion (standard deviation) were presented for quantitative variables and absolute frequencies and percentages were presented for categorical variables. Additionally, the relationship between the intraoperative variables (operative time, conversion, complications, and simultaneous surgeries) and the recurrent risk of fistula was analyzed. Student's t-test was utilized to contrast quantitative variables. A χ2 test or Fisher's exact test was applied to categorical variables. A value of p < 0.05 was considered significant.
Results
Most patients were between 39- and 48-years-old (58.3%), and the oldest was age 80. Most patients were without surgical risks. Abdominal hysterectomy was the most frequent cause of VVF (94.4%). Most patients had only one fistula orifice. Delayed repair was performed in all patients, one obstetric VVF was repaired 25 years after the lesion appeared, and 13.8% were recurrent (previous surgeries were performed via an open surgical approach). Table 1 shows the various characteristics of the patients and the perioperative results are presented in Table 2. Operative time was excluded in 4 patients who had other simultaneous surgical procedures. These included JJ stent placement due to ureteral orifice stenosis and ureteroscopy to dilate distal ureteral stenosis, hysterectomy and cholecystectomy due to cholelithiasis in a patient with a fistula of obstetric cause; and nephrectomy because of renal function loss due to a combined lesion of the ureter in a recurrent VVF that had been previously repaired by open abdominal surgery.
There were three recurrences; one of them was treated by electrofulguration with argon plasma, while two required open surgery. One of them recurred again.
There were no intraoperative complications. Postoperative complications included an infected pelvic hematoma with sepsis requiring reintervention with abdominal lavage using a laparoscopic approach, as well as blood transfusion, antibiotic therapy, and intensive care. The fistula closed despite this complication. Urine drainage through the peritoneal tube (the Nelaton catheter), routinely placed into the Douglas cul-de-sac, was prolonged in 2 patients, and both required replacement of the ureteral catheters. One patient had an infrequent complication—acute renal failure due to obstructive anuria after the ureteral catheters were withdrawn; she was treated by reinserting the ureteral catheters. All complications were Dindo classification Grade IIIb.
Biopsy of the fistulous tract was negative for malignancy in these patients.
The intraoperative variables and the fistulae recurrence risk were analyzed. Three patients with recurrent fistulae had no simultaneous surgeries (8.3%), p = 0.630. Operative time in patients with recurrent fistula was less (120.0 minutes), with respect to the patients without recurrence (152.2 minutes), but these differences were not significant at p = 0.306. Other intraoperative variables (conversions and complications) were not reported.
Discussion
VVF affects middle-age women between the fourth and fifth decade of life. Most articles on series, particularly those related to laparoscopic repair, report a similar average age.1,8
In developing countries, obstetric accidents are the most frequent cause of VVFs, whereas, in developed countries, it is abdominal hysterectomy, particularly related to myomas, most frequently performed by open surgery. Other causes are abdominal radical hysterectomy, surgery for endometriosis, and total laparoscopic hysterectomy.9–13
Preoperative assessment by an anesthesiologist is an essential component for comprehensive care and safety of the patients who will undergo any surgery. Some characteristics of laparoscopic surgery increase the risk of some complications, such as venous thromboembolism (VTE). This risk is higher if the surgery exceeds 60 minutes, and is related to gynecologic position, prior or concurrent pelvic surgery, being over 40 years of age, and obesity. Even though some patients in the series had comorbidities, VTEs did not occur, and this was probably related to the prophylaxis protocols followed at the National Center for Minimally Invasive Surgery.14,15
Complications, especially those related to urinary-tract lesions, are most frequent in laparoscopic hysterectomies, although, in this series, this cause was minimal. The National Center for Minimally Invasive Surgery reported 0.7% bladder lesions in 1599 hysterectomies, which is lower than other international reports and is probably due to the strict observation of the technical details of the surgery, its standardization, and having a multidisciplinary team that involves close relationships among the departments of surgery, gynecology, and urology. 16
The mean size of the VVF was somewhat larger in this series (Table 1). In other reports, other VVF series repaired with minimal invasiveness had a mean size a little over 1 cm.17,18
A controversial aspect is the time interval required between the appearance of the VVF and its surgical repair. Typically, it has been established between 3 and 6 months. There is no consensus as to what time is considered delayed or early in VVF repair. Closure from 1–3 months is usually considered early, and, from 3 months on, it is considered delayed.19,20
Typical management has been to delay surgery until 3–6 months later. Some researchers find no benefits in postponing VVF closure. They recognize that early closure reduces physical and mental discomfort, but recommend a careful selection of patients that balances the possibility of not compromising the success of the surgery, in which early repair has been reported as between 86% and 100% in small series. 21
Nevertheless, when fistulas appear late after surgery due to ischemia, the medical literature suggests to wait several months. Currently, the fact that understanding of VVF etiology is different from the past has led to the criteria of early surgical treatment. However, it is beneficial to delay surgery until tissues improve and infection is under control, especially in VVFs of obstetric causes.9,21,22
The current authors have not considered immediate VVF closure. Average time intervals for surgery in other series have been similar. The fact that a patient had surgery after having had a lesion for 25 years is intriguing. She came from a rural area and said she had been treated for sclerosis and had not received any information about a surgical option. In the series presented by Singh et al., a patient also came for surgery 13 years after her lesion appeared. 23
Primary closure is associated with better results. Most patients had primary closure, but prior previous attempts at surgical repair were not obstacles to the laparoscopic approach. The antecedent of prior abdominal open surgery for VVF repair—taking into consideration that the patients had had at least two abdominal surgeries before laparoscopic repair—was not a contraindication. Prior attempts at repair of a VVF makes the surgery more arduous due to the presence of peritoneal adhesions, but, as has occurred in other work groups with experience in laparoscopic surgery, it can be successfully performed without complications.24,25
The use of a third tissue layer with omentum is recommended in the closure of a secondary fistula. It has been demonstrated that the number of previous repairs is not an independent predicting factor for the interposition of other tissues in the repair, as had been suggested up to now. Each patient should be analyzed individually in order to make this technical decision. 26 The operative time for VVF repair in the current study was similar to that in other series.11,23
Despite being an arduous surgical technique that requires experience in intracorporeal sutures performed in patients with previous abdominal surgeries, and simultaneous surgical laparoscopic procedures, no conversion to open surgery was required. Some series did not report conversions and others reported low rates.10,22,23
Hospital stay in open and laparoscopic surgery for VVF repair has shown significant differences in favor of laparoscopic surgery. Length of hospital stay in other series is shorter than in this series. The longer stay was due to prolonged urine leakage through the peritoneal tube (the Nelaton catheter) that is routinely placed into the Douglas cul-de-sac, and related to a defect in the vesical suture at the beginning of the series. Therefore, this corresponded to the learning curve for intracorporeal suturing and the fact that external ureteral catheters are maintained routinely after surgery. In those circumstances, the current authors do not recommend early discharge. Other researchers have reported a usual stay of 1–3 days. 11
Out of five associated surgical procedures, two were related to the presence of complex fistulae with ureteral involvement that could be treated with endourologic procedures such as JJ stent placement and ureteroscopy. Three were laparoscopic procedures for nephrectomy, hysterectomy, and cholecystectomy. Associated procedures are considered those that are performed simultaneously to treat different surgical pathologies. Working in a multidisciplinary group, which is how surgery is carried out in this institution, allowed the surgeons to address different pathologies safely. There are advantages of having only one anesthetic treatment and benefits of only one postoperative recovery from concomitant surgically treated diseases, with concomitant economic advantages. Some guidelines for success have been established, such as correct preoperative assessment, a well-supported indication, and the observation of certain technical aspects that guarantee success. These include an appropriate decision regarding entry ports, degree of contamination assessment, technical complexity, contraindications, estimated operative time, and learning curve of the specialties involved. 27
There were no complications, reinterventions, or lengthening of hospital stays, nor was the success of VVF repairs compromised in patients who had associated surgical procedures.
There have been few complications reported for laparoscopic VVF repair. Some researchers have not even reported complications.11,22
Complications of surgical VVF repair have been reported, such as recurrent fistula formation, vaginal stenosis, reduced bladder capacity, irritative lower urinary-tract symptoms, and ureteric injury or obstruction. 28
The complications produced in this series were resolved with minimally invasive methods.
Surgical treatment has shown to be more successful for repair of VVF than conservative treatment, and thus surgery is considered the first line of treatment. The laparoscopic approach has evidenced the same high success rates as abdominal open surgery. The success rate in one of the largest series was 86%, whereas in a multi-institutional series, it was 95.2%. Miklos et al. 29 published a success rate between 95.5% and 98.04% for transvesical and extravesical laparoscopic techniques, respectively.11,22,29–31
The results of laparoscopic surgery for VVF were similar to those reported by some researchers who used a vaginal approach.11,31
With respect to the use of ureteral catheters, few researchers extend its use postoperatively. This is opposed to the current authors' usual practice, in which it is considered wise to keep them for at least 3 days, or more in the cases with prolonged urine leakage through the abdominal tubular drainage. Satisfactory, successful results are achieved.18,22
The current authors have been conservative regarding the time of removal of the urethral catheter, showing a higher time of removal average than other researchers. Others withdraw it after an average of 24.4 days and show a range of 18–34 days, while less time has been reported.11,13,18
There was no evidence that the intraoperative variables analyzed—operative time, and performance of simultaneous surgeries—were related to VVF recurrence risk, with values of p = 0.306 and p = 0.630, respectively.
Conclusions
The advantages of the laparoscopic approach, compared to open surgery, include magnification of the surgical field, better hemostasis, and shorter hospital stay and recovery. 6 Repair of VVFs with laparoscopic surgery is an effective and safe procedure, with a high success rate, and is an alternative in the treatment of VVF.
Footnotes
Acknowledgments
The authors would like to acknowledge Berta Moinelo Plasencia, BA, for reviewing the English version of this paper and the staff of the National Center for Minimally Invasive Surgery, for their participation in the study.
Dr. Tania González León, the surgeon of all the cases and the first author of this article, would like to acknowledge other authors from her institution and from other institutions for participating in the data collection and writing of this article.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.