
Abstract
Abstract
Introduction
E
Case
A 35-year-old parous woman presented to the urogynecology clinic of the KK Women's and Children's Hospital, Singapore, with a lump arising through her vagina since a normal vaginal delivery 4 years prior. She had no difficulty passing urine. Her menstrual cycles were regular with normal flows and no dysmenorrhea. She did not complain of dyspareunia. On examination, a 4 × 4 cm vaginal cyst was noted in the lower one-third of the vagina on the left lateral side, close to an episiotomy scar (Fig. 1). The cyst was fluctuant and nontender on touch. There were no other significant findings on examination. She was counseled to undergo excision of the cyst and she consented to do so. The procedure was performed under general anesthesia. The cyst wall was inadvertently ruptured during the procedure, and a thick chocolate-colored fluid poured out from within the cyst. The cyst wall was excised and the dead space and vulval skin were closed using a Vicryl Rapide

Left-sided Bartholin's cyst. Color images available online at www.liebertpub.com/gyn
Results
The patient was given postoperative antibiotics and recovered well. The histopathologic examination was consistent with a Bartholin's cyst with endometriosis and no evidence of malignancy. There were foci of sheets of pigment-laden macrophages beneath the lining epithelium. Some of these foci showed positivity for CD10 (Figs. 2–4).
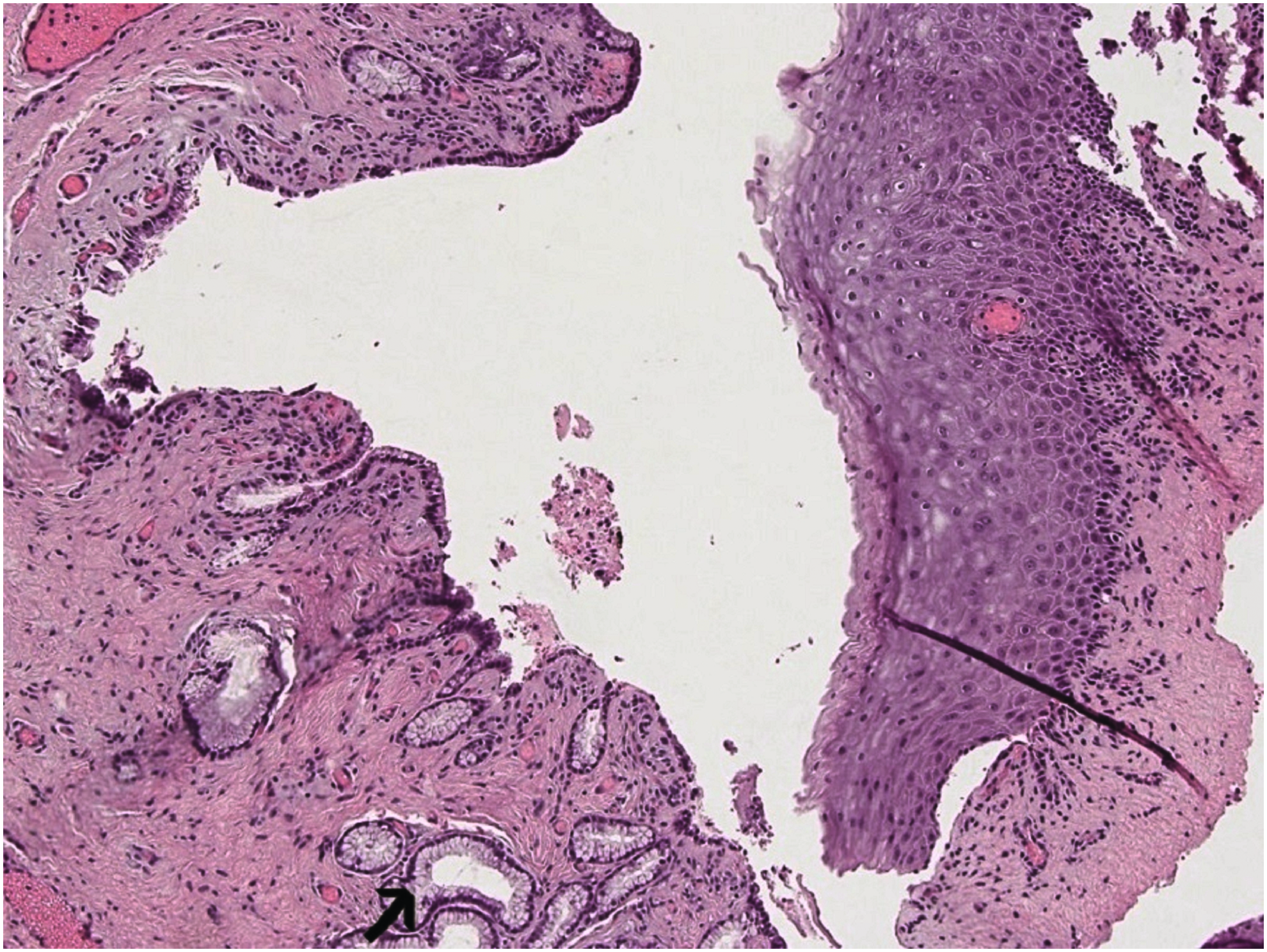
High-power magnification showing seromucinous glands of Bartholin's cyst (arrow). Color images available online at www.liebertpub.com/gyn

High-power magnification showing endometriotic deposits with foam cells and macrophages (arrow). Color images available online at www.liebertpub.com/gyn
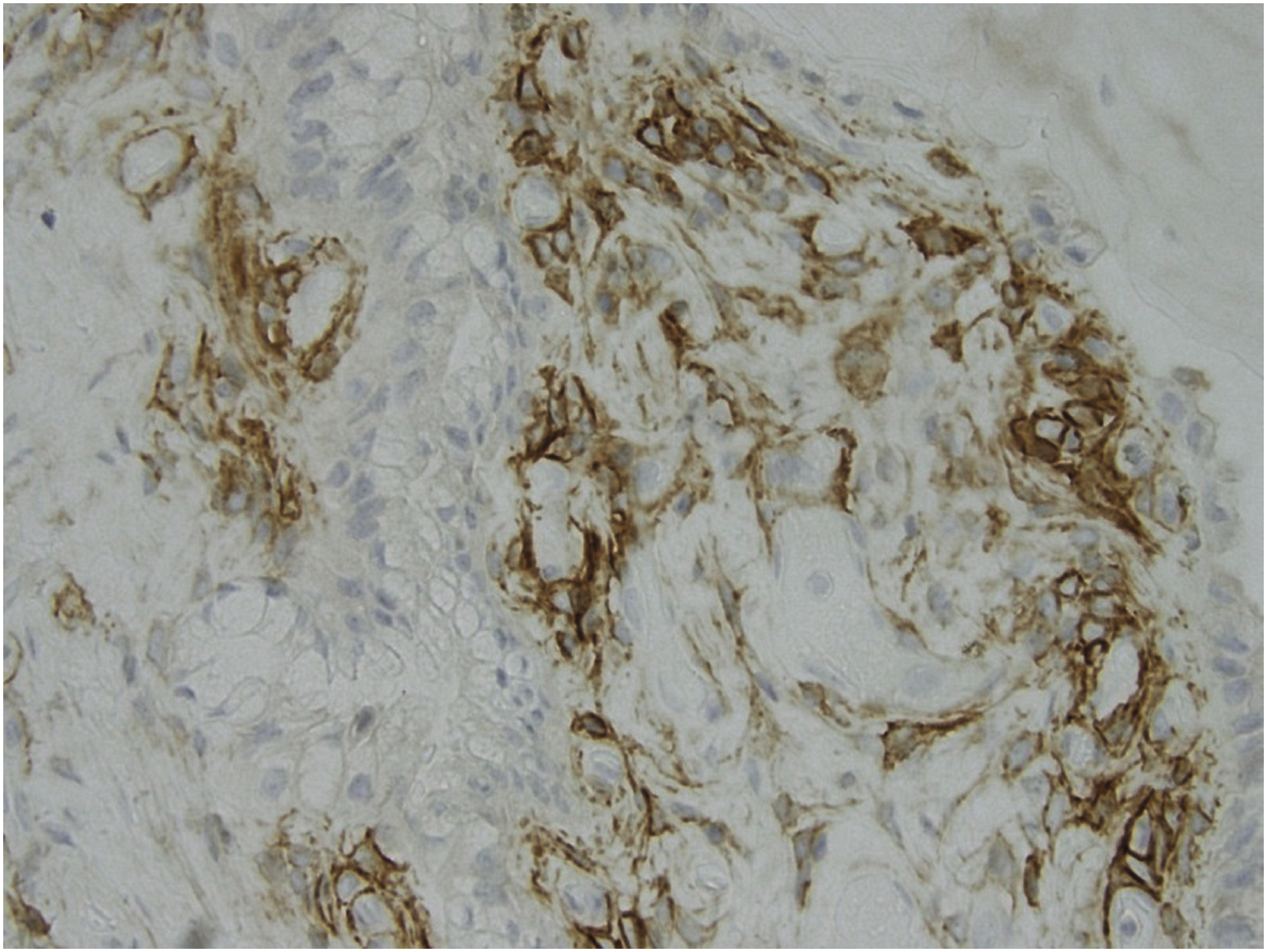
Endometriotic focus within the Bartholin's cyst showing CD10 positivity. Color images available online at www.liebertpub.com/gyn
Discussion
The most popular present theory of the origin of endometriosis is the Sampson's theory of retrograde menstruation, according to which, the ectopic endometrium flows in a retrograde fashion through the fallopian tubes into the peritoneal cavity during menstruation and forms implants. 7 The origin of extrapelvic endometriosis is not well-deciphered. Presence of endometriosis in the labia majora can be explained by the direct spread of pelvic endometriosis along the round ligaments. A solitary focus in the Bartholin's gland may theoretically be attributed to coelomic metaplasia or spread along lymphatic or vascular channels. Endometrial bits of tissue that have reached the Bartholin's glands through their openings at the introitus may grow under the influence of hormones.1,8,9
Extrapelvic endometriosis may cause unique symptoms. The symptoms are often cyclical, with about half of these patients reporting periodic variation in the sizes and tenderness of the implants.1,9 This condition is often diagnosed coincidentally during surgery for a different indication or during histopathologic examination. 9
Sośnik et al. conducted a study published in 2007 in which 104 Bartholin's glands surgically excised from 103 female patients, 39.4 ± 9.6 years' old, for various indications were examined histopathologically. Two percent of these specimens showed endometriotic deposits. 10 Aydin et al. reported a case in which endometriosis was found in bilateral Bartholin's glands in a patient with ovarian endometrioma. 8 The presence of extrapelvic endometriosis has also been reported in episiotomy scars. A possible explanation is the autologous transplantation of endometrial tissue to the episiotomy scars during vaginal delivery.3,11,12
Fine-needle aspiration of the lesion may help in diagnosis but cannot be used as a treatment measure as it is not efficaceous. 2 The specimen might often be nondiagnostic, as it may be difficult to differentiate extensive cytologic atypia from carcinoma. 5 The optimal management of endometriosis in the perineal area is wide surgical excision of the lesion. The risk of recurrence is high if the lesion is not completely excised. There is a likelihood of transformation of endometriosis into malignancy. Surgical excision of the lesion helps in obtaining a histologic diagnosis and also in excluding malignancy8,9,4 Patients should be followed-up postoperatively to monitor for any recurrence of such lesions. 3 Malignancy arising from endometriotic deposits in the vulva has been reported in the literature.13,14
The medical management options for extrapelvic endometriosis include oral contraceptive pills, progestogens, gonadotropin-releasing hormones, and danazol. These medications are not very beneficial, as they do not provide complete relief of symptoms and do not ablate the lesions.4,5,15
Conclusions
Vulvar endometriosis should be considered as a possible, although rare, cause of cystic masses of the vulva, especially those associated with variability in size and tenderness during the menstrual cycle. Symptoms and clinical examination alone cannot lead to a diagnosis of extrapelvic endometriosis conclusively. Surgical excision and histopathologic examination is necessary to establish a definitive diagnosis.
Footnotes
Author Disclosure Statement
None of the authors have any conflicts of interest.