
Abstract
Abstract
Objectives:
Neoadjuvant chemotherapy is being used increasingly prior to debulking for ovarian serous carcinoma. There can be significant histopathologic alterations, sometimes making the pathologic diagnosis challenging.
Methods:
A MEDLINE search was performed, and articles describing the histologic changes associated with neoadjuvant chemotherapy, as well as any possible clinical impact, were reviewed.
Results:
The scope of histopathologic changes seen after neoadjuvant chemotherapy for ovarian serous carcinoma, as well as their possible clinical significance, is presented. Histopathologic changes included degenerative changes, increased atypia, and alterations that can make pathologic interpretation difficult, particularly if there is a lack of familiarity with these changes and lack of an available clinical history.
Conclusions:
More research is needed to assess whether or not there is any prognostic significance to these alterations. (J GYNECOL SURG 33:1)
Introduction
N
Methods
A MEDLINE® search was performed, and articles describing the histologic changes associated with neoadjuvant chemotherapy, as well as any possible clinical impact, were reviewed.
Results and Discussion
The mainstay for many years for initial therapy for high-grade serous epithelial ovarian carcinoma has been optimal debulking. Total or optimal debulking (<1 cm of residual disease) is the best prognosticator of survival. 1 Conventionally, debulking has been followed by chemotherapy. However, with advanced-stage disease, optimal debulking at initial presentation may not be feasible, and neoadjuvant chemotherapy, wherein several cycles of chemotherapy are given prior to the initial surgery, may make debulking more achievable. This is now an acceptable alternative approach. 2 Prior to more widespread use of adjuvant chemotherapy for cytoreduction prior to debulking, it was noted in occasional cases that histopathologic alterations occurred that might make interpretation difficult.
In a small series of patients with serous and endometrioid ovarian carcinomas, McCluggage et al. 3 noted single-tumor cells or small tumor-cell clusters within a fibrotic stroma. The tumor cells had undergone pronounced cytologic changes, making tumor grading and typing difficult to impossible. These included nuclear enlargement, hyperchromatism, and a “smudgy” appearance, as well as changes in the cytoplasm, such as eosinophilia, vacuolization, and foamy changes. Background changes included fibrosis, inflammation, foamy histiocytes, cholesterol clefts, hemosiderin, calcification, necrosis, and abundant psammoma bodies. 3 See Figures 1–3. In addition to difficulties in typing and grading tumors, these researchers observed that numerous sections, as well as immunohistochemistry, could be required to even establish the presence of a tumor.
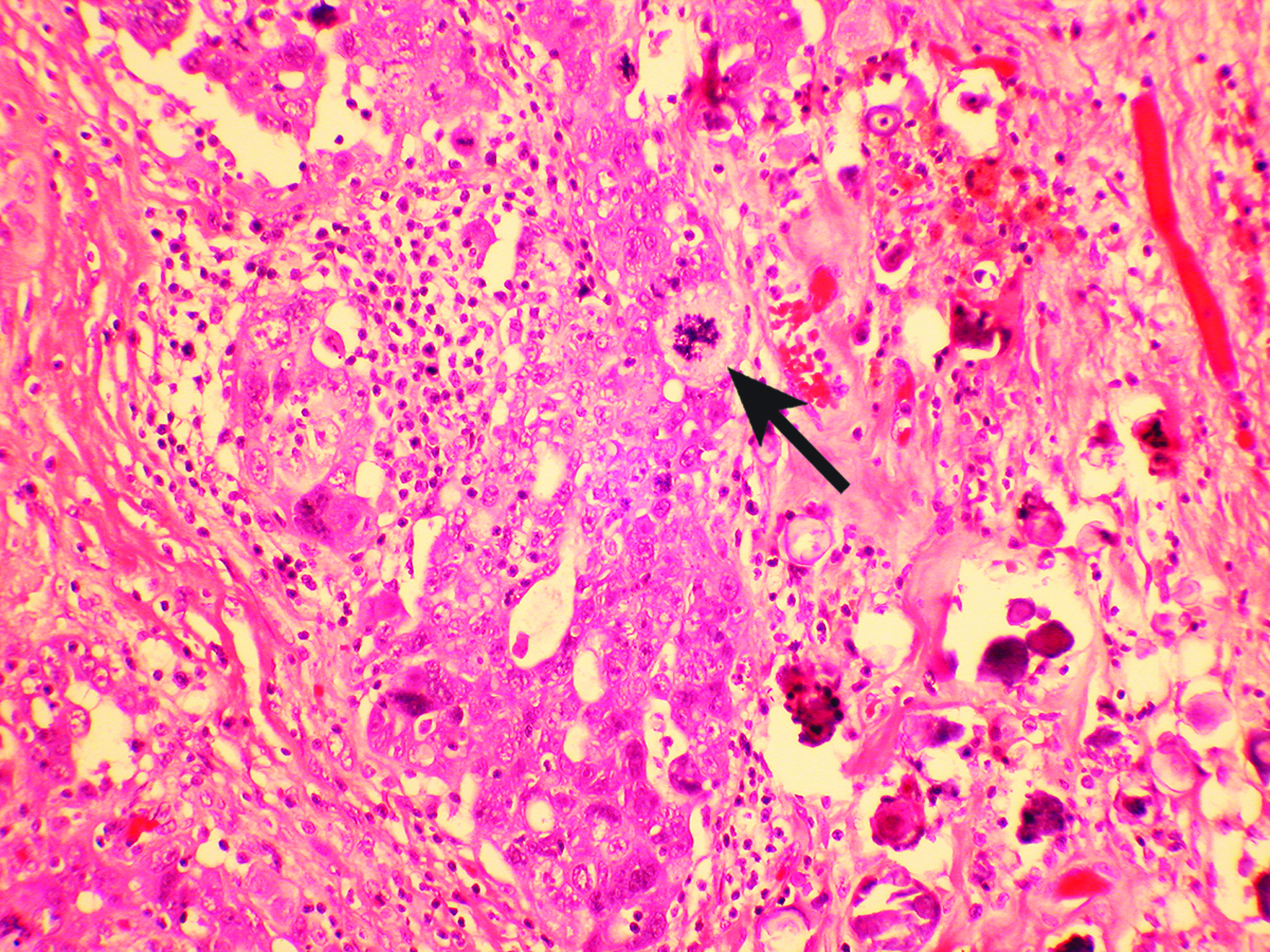
Cluster of tumor cells in the center of the image. Nuclei are often smudged and difficult to interpret. An atypical mitosis is seen (arrow). A background of chronic inflammatory cells is seen at the center. To the right, numerous psammoma bodies are present. Color images available online at www.liebertpub.com/gyn
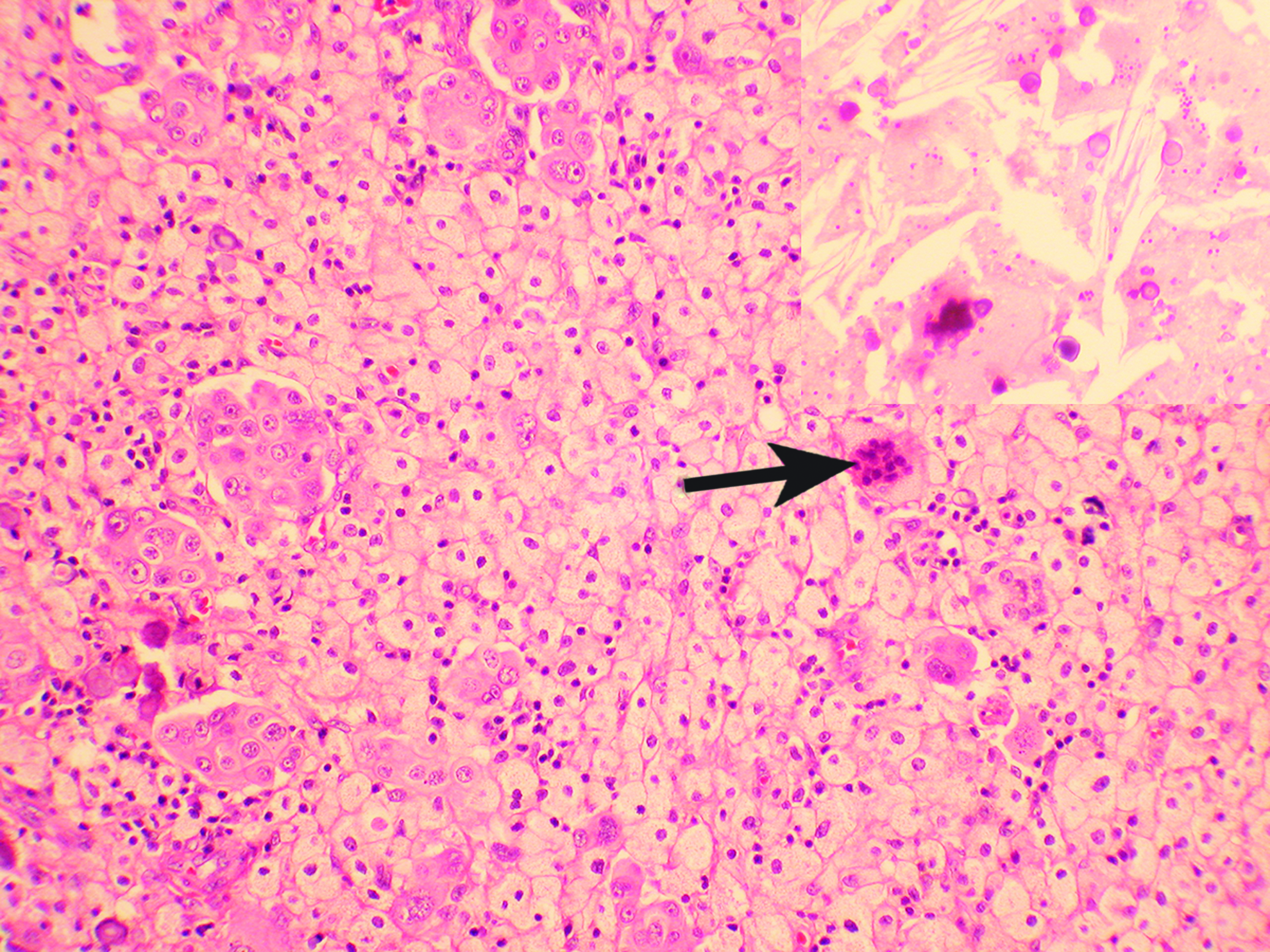
Small clusters and single tumor cells, some multinucleated; multinucleated foreign-body giant cells (arrow) in a background of foamy histiocytes. Other areas showed numerous calcifications, and cholesterol clefts (inset). Color images available online at www.liebertpub.com/gyn
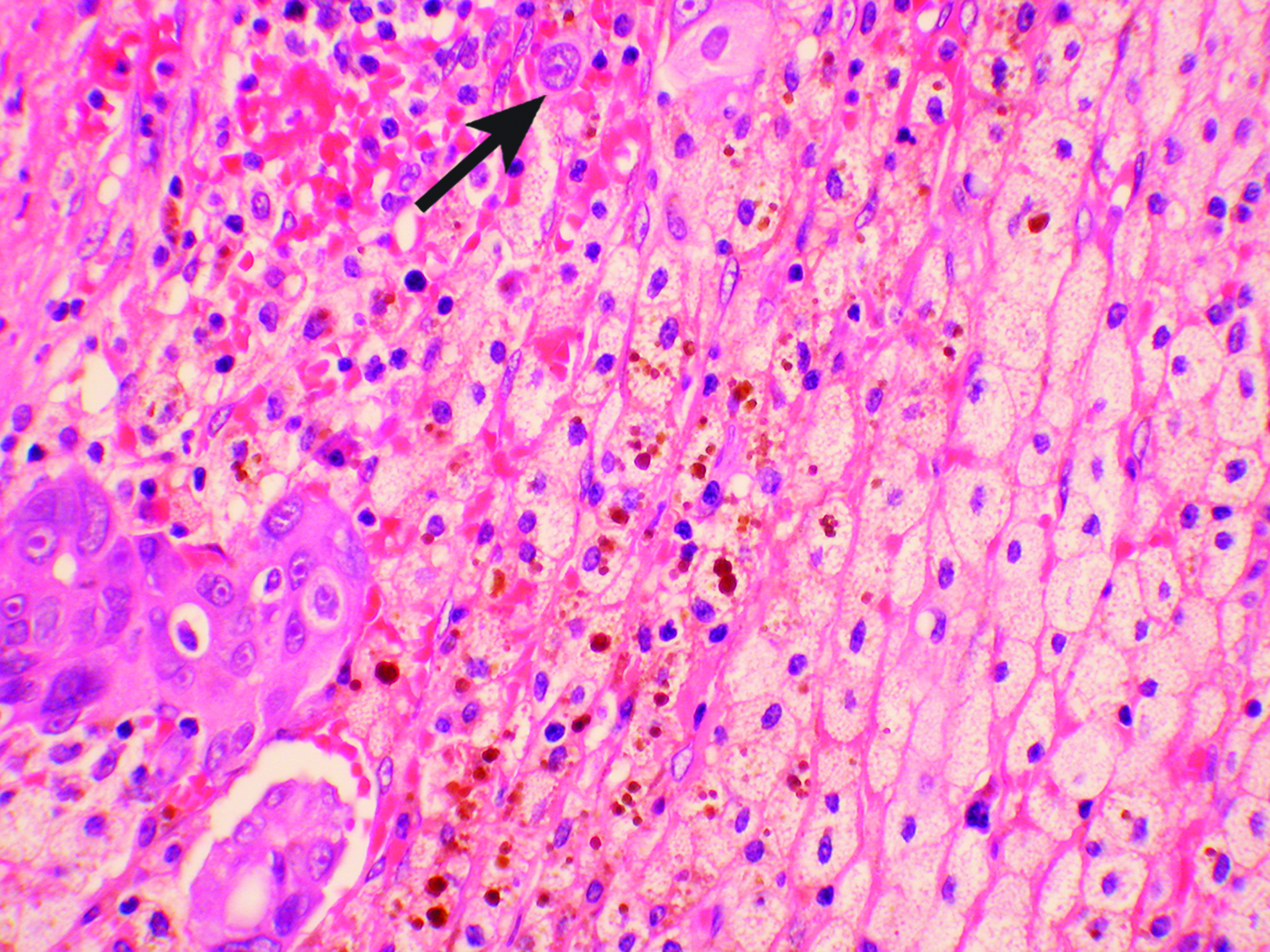
A cluster of tumor cells (lower left) with scattered smudged nuclei amid reactive nuclei, single tumor cells (arrow), hemosiderin brown pigment, and sheets of foamy histiocytes are present in some fields. Color images available online at www.liebertpub.com/gyn
The risk of overdiagnosing clear-cell carcinoma when cytoplasmic vacuolization is seen has been noted,3,4 with one report cautioning clinicians about the risk of diagnosing a mixed carcinoma or second carcinoma. 4 Utilizing a panel of immunohistochemical stains has been proposed as an aid to diagnosis 5 ; this was suggested as particularly helpful if a prior history of ovarian carcinoma was not available or the cytologic changes were pronounced. Inappropriate workup and therapy may be avoided in this manner. 5 Suggested stains in this panel included estrogen receptor (ER), p53, WT1, PAX8, CK7, CK20, and CDX2. Ovarian serous carcinoma often stain for ER, p53, WT-1, PAX-8, and CK7, and occasionally for CK20, which is more often positive in colon cancers, which are also positive for CDX-2. 5 The researchers also suggested that diagnosis was aided in these challenging cases by good clinician–pathologist communication.
In paired studies of pre- and postchemotherapy serous carcinoma, the immunoprofile has been shown to be maintained. 6 A scoring system for the histologic changes has also been proposed. 2
Recent literature has indicated that serous carcinoma of the ovary and peritoneum might actually originate in the tubal fimbria. In a study by Colón and Carlson, 7 serous tubal intraepithelial carcinoma, the putative precursor lesion, was shown to persist after neoadjuvant chemotherapy, as was the p53 signature, the initial genetic aberration demonstrable by immunohistochemistry. These findings may assist in diagnosing challenging cases, particularly if indepth evaluation of the fimbria—such as is performed in prophylactic salpingo-oophorectomies for BRCA mutations (the SEE-FIM protocol)—is conducted, an evaluation that these researchers recommend for neoadjuvant cases. 7
Whether or not any of the histopathologic findings seen after neoadjuvant chemotherapy signify an improved prognosis has been a topic of interest for a variety of nonovarian solid tumors, including those of the breast and lung. 8 The literature on ovarian carcinoma is controversial. A small amount of literature on the prognostic significance of neoadjuvant chemotherapy in ovarian carcinoma has emerged. In one study comparing the histology of tumors that were primarily resected versus resection after neoadjuvant chemotherapy, significant histopathologic alterations after neoadjuvant chemotherapy included single-tumor cells, fibrosis, foreign-body giant cells, and foamy macrophages, 9 which were found to be of high specificity but low sensitivity. Less specific were inflammatory changes, hemosiderin, and psammoma bodies. Interestingly, necrosis was more highly associated with larger tumor size, and, hence, was more likely to occur in the controls than in the patients who underwent resection after chemotherapy in this series. Only tumor size—and no specific pathologic changes—correlated with longer median survival in this series, with either no tumor, tumor single cells, or tumors 5 mm or less consistent with significant responses. 9 The researchers noted that all these regressive findings—as well as tumor giant cells—could be also be seen in untreated cases.
In contradistinction, Le et al. showed that lack or minimal necrosis after neoadjuvant chemotherapy was an independent risk factor for recurrent disease. 10 The researchers acknowledged the difficulty in assessing necrosis as well as the limitations involved in a small retrospective study. 10 In a subsequent retrospective study, 11 a grading system was created that included necrosis, fibrosis, macrophages, and inflammation; this composite tumor-response scoring was prognostic for time-to–disease-related death. However, Ferron et al. 12 found that even no histologic residual disease did not predict overall survival reliably—although this result did correlate with 3 year event-free survival—and was not a good indicator to use when planning chemotherapy after debulking.
Conclusions
Future and larger prospective studies will be helpful for assessing the utility of histopathologic findings after neoadjuvant chemotherapy in prognostication. One advantage to establishing histopathology of interval surgery as a prognostic factor would be that it could be available earlier than clinical markers of disease progression, including CA-125 and imaging. 2 This might aid in earlier interventions, including additional chemotherapy or additional debulking procedures. In addition, the histologic findings after neoadjuvant chemotherapy can be challenging to recognize. Pathologists need to be aware of the range of histologic alterations when evaluating these specimens to arrive at the correct diagnosis. Clinician–pathologist communication is important in these difficult cases.
Footnotes
Author Disclosure Statement
The authors have no disclosures to report.