
Abstract
Abstract
Background:
An uncommon condition known as pyometra occurs when natural drainage of the uterine cavity is compromised and pus accumulates within the cavity. The reported incidence is 0.1%–0.5% in gynecologic patients and is much higher in elderly women. Spontaneous perforation of pyometra and subsequent diffuse peritonitis is very rare.
Case:
A postmenopausal (age 60, para 3) woman presented in an emergency department with fever and pain in her abdomen. Features of generalized peritonitis were present on examination. Laparotomy was performed, and a rent with pus leaking from it was found on the anterior wall of the uterus. Subtotal hysterectomy with bilateral salpingo-oophorectomy with cervical cytology was performed.
Results:
There was no evidence of malignancy on histopathology and cytology examination. Pyometra was caused by senile endometritis, and pus was not expelled out because of cervical stenosis. This case had an unusual presentation in the form of a rupture of pyometra with subsequent development of peritonitis.
Conclusions:
Spontaneous uterine perforation caused by pyometra should be kept in mind as one of the differential diagnosis in a postmenopausal woman presenting with generalized peritonitis. Clinicians usually miss the diagnosis of rupture of pyometra in a previously asymptomatic elderly female; this report will help create the awareness to avoid this life-threatening condition. (J GYNECOL SURG 33:71)
Introduction
A
Spontaneous perforation of pyometra and subsequent diffuse peritonitis is very rare, with an incidence of 0.01%–0.05%. 4 More than 50% of patients with unruptured pyometra are asymptomatic. 5 Once pyometra is ruptured, a patient develops an acute abdomen and generalized peritonitis. 4 The report is about a patient who was admitted to the Pt. B.D. Sharma, Postgraduate Institute of Medical Sciences (PGIMS), in Rohtak, Haryana, India, for diffuse peritonitis caused by a spontaneously perforated pyometra.
Case
A 60-year-old female, para 3, presented in the emergency ward with a complaint of fever for 7 days and pain in her abdomen for 3 days. She was referred to the PGIMS tertiary health care institute from a private hospital. She had been menopausal for the last 10 years. Her fever was associated with chills and rigor and was relieved by medication. Her pain was severe in intensity, was referred to her back, and was aggravated by movement. She denied any history of postmenopausal bleeding or discharge per vaginum. She had an ultrasound report that showed a senile uterus that was distended with echoes suggestive of pyometra and a collection with echoes in the abdominopelvic region measuring 130 × 11.5 mm, extending in the bilateral adenexa. There was a tubo-ovarian abscess.
On examination, this patient was conscious but disoriented. She was afebrile at that time. Her pulse rate was 106 beats/minute, her blood pressure was 100/70 mm Hg, and her respiration rate was 18 breaths/minute. On chest examination, it was noted that bilateral air entry was decreased.
The patient's abdomen was distended, tense, and tender, with guarding and muscular rigidity. Bowel sounds were absent and no definite mass was palpable. Per speculum examination revealed a cervix that was flush with the vagina and pus leaking through the os. On bimanual examination, the uterine size could not be determined, and fullness was present in all of the fornices.
Laboratory investigations were: hemoglobin, 10 gm%; total leukocyte count, 22,000/mm3; differential leukocyte count, 90%N, 8%L, 1%M, 1%E; platelets, 1.7 lac, blood urea, 47 mg/dL; serum creatinine, 1.7 mg/dL, blood sugar, 72 mg/dL, serum sodium, 117 meq/dL; serum potassium, 4.2 meq/dL; INR-1.27; and a Widal test produced negative results. An X-ray of her abdomen was taken in view of suspected gut perforation or uterine perforation, but the X-ray did not show air under the diaphragm. A chest X-ray revealed a bilateral pleural effusion; thus, a pleural tap was performed.
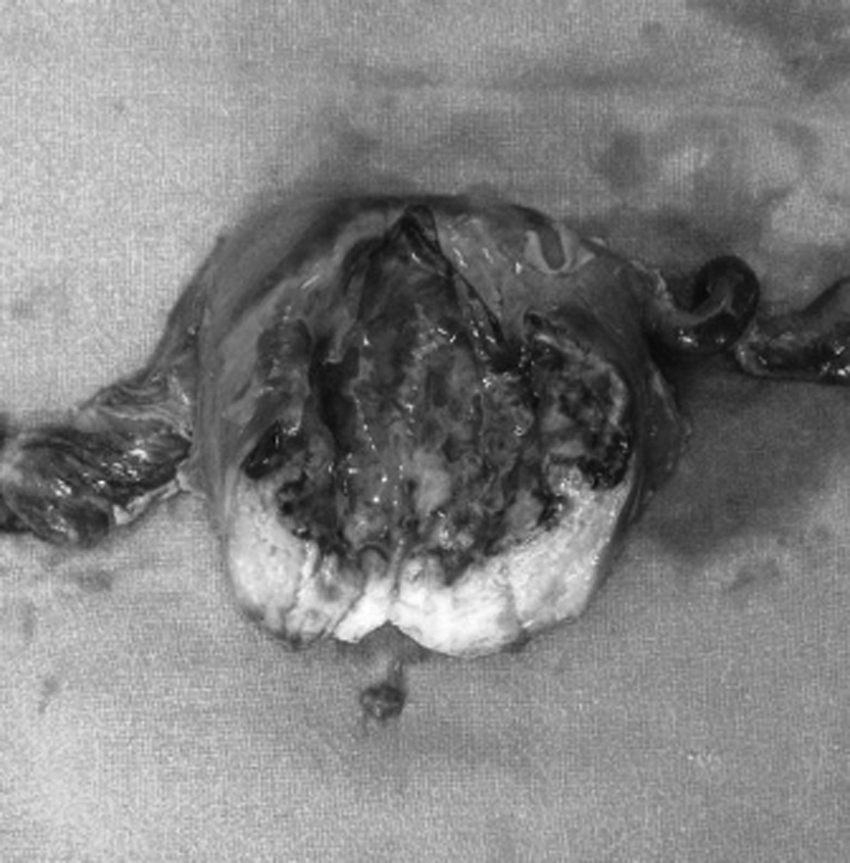
Broad-spectrum antibiotics were started. A nasogastric tube was inserted and 1000 mL of green-colored secretions were aspirated. In consultation with a surgeon, an emergency laparotomy was performed. Preoperatively, her gut loops were dilated and adherent to each other. Omentum was covering all the gut loops. On separating the omental and gut adhesions, 300 mL of foul-odored pus was found in the peritoneal cavity; this pus was drained and sent for culture sensitivity testing. There was no abnormality in the alimentary tract. Pus flakes were adherent to the gut serosa and uterus. On exploration of the uterus, it was noted that there was a 2 × 1–cm rent on the anterior wall of the uterus, pus was coming out of this rent (Fig.1). The Uterus was 8 weeks in size and was gangrenous around the rent. Bilateral parametria were inflamed and thickened and the bladder was adherent to the uterus.

Uterus showing perforation.
Results
A subtotal hysterectomy with a bilateral salpingo-oophorectomy was performed. A cut section of uterus revealed necrotic endometrium (Fig. 2), and a specimen was sent for histopathologic examination. Postoperatively, a Papanicolaou smear was taken and sent for cytology examination. Intensive monitoring lasted for 48 hours and the patient was discharged on the seventh postoperative day in a healthy state. Histopathologic examination revealed pyometra with no evidence of malignancy. The cervical cytology report showed dense inflammation.
Cut section of the specimen.
Discussion
Pyometra is the collection of pus or a mixture of pus and blood inside the uterus. Stenosis of the cervical canal in carcinoma of the cervix, carcinoma corporis, operations on the cervix, radiotherapy, senile endometritis, puerperal endometritis with retention of lochia, and tubercular endometritis are some of the common causes of pyometra.6–10 Patients usually present with symptoms of purulent vaginal discharge, suprapubic pain, and postmenopausal bleeding or spotting, 11 but, in the present case, the patient was asymptomatic until she presented with an acute abdomen. After menopause, when the endometrium loses its resistance and does not shed cyclically, any infection that enters inside the uterus can persist as senile endometritis. The atrophic endometrium is destroyed and converted into granulation tissue. There is formation of pus, which gets collected inside the uterine cavity. The pus is not expelled out of cervical canal because of narrowing or fibrosis of the cervix and poor myometrial contractility. The uterus enlarges by thinning its walls, and spontaneous rupture occurs resulting in peritonitis. No obvious cause was identified in this case, so postmenopausal changes and cervical stenosis could be the probable causes. Senile endometritis presenting as pyometra requires cervical dilatation and drainage of pus, but this case had an unusual presentation in the form of a rupture of pyometra with subsequent development of peritonitis.
The organisms responsible are coliforms, streptococci, or staphylococci, and they are rarely tubercular. 12 In the current case, Staphylococcus aureus was isolated. In an extensive study by Yildizhan et al., the site of perforation was the uterine fundus in 85.7% of the cases. 13 In the present case, the perforation was on the anterior wall of uterus.
It is difficult to diagnose this condition preoperatively because of nonspecific symptoms. Definitive diagnosis is made on laparotomy as in the present situation. Peritonitis secondary to rupture of pyometra should be considered as a surgical emergency, and immediate laparotomy must be performed to avoid complications of generalized peritonitis. Septic shock is one such life-threatening complication. Total abdominal hysterectomy with bilateral salpingo-oophorectomy is the ideal choice of definite surgery. In cases of ruptured pyometra, if one performs supracervical hysterectomy, carcinoma of the cervix—which is a common cause of cervical stenosis—might be present, thereby pyometra can be missed. Supracervical hysterectomy is easier to perform than total hysterectomy and, in certain situations—such as adherence of the bladder or the presence of inflammation—total hysterectomy may not be possible, as occurred in the present case. Cervical cytology testing was performed to rule out carcinoma of the cervix.
Conclusions
Spontaneous uterine perforation caused by pyometra should be kept in mind as one of the differential diagnosis in a postmenopausal woman presenting with generalized peritonitis. Early diagnosis and intervention is required to reduce morbidity and mortality. Clinicians usually miss the diagnosis of rupture of pyometra in a previously asymptomatic elderly female; this report will help created the awareness to avoid this life-threatening complication.
Footnotes
Acknowledgment
This case report was supported by the Department of Obstetrics and Gynaecology, of the Pt. B.D. Sharma, PGIMS, in Rohtak, Haryana, India.
Author Disclosure Statement
There are no conflicts of interest.