
Abstract
Abstract
Background:
Scar endometriosis is a rare entity of endometriosis with an incidence of <1%.
Case:
A 39-year-old woman developed scar endometriosis on top of a Pfannenstiel incision and that invaded her rectus sheath. This patient's condition was initially misdiagnosed as an incisional hernia. She was found to have a mass, which was excised surgically and sent for histology testing.
Results:
Histopathologic testing revealed that this patient had scar endometriosis. A postoperative follow-up at 18 months showed that she had an uneventful recovery.
Conclusions:
Scar endometriosis is a rare and deceptive condition that might mimic an incisional hernia, thus, requiring a high level of suspicion. A multidisciplinary approach is essential for reaching the correct diagnosis especially in atypical cases. (J GYNECOL SURG 33:74)
Introduction
E
The local institutional review board of As-Salam International Hospital, in Cairo, Egypt, approved the publication of this case report.
Case
Scar endometriosis developed in a 39-year-old woman 15 months after she had had a third cesarean section. She presented with a painful firm swelling of limited mobility on top of a Pfannenstiel incision; this swelling was noticed by the patient since her last delivery. Her pain and swelling had increased over the last 3 months, prior to presentation, especially during menses (she had had lactational amenorrhea for 1 year). The pain and swelling made her seek medical advice because this was the first time in her life that she had experienced such pain. She had no previous history of endometriosis. The mass was initially diagnosed as an incisional hernia. However, this patient's vague history and atypical findings on examination warranted further investigation, but magnetic resonance imaging was not available. Thus, computed tomography (CT) scanning was performed. The CT scan showed a mass invading the rectus sheath (Fig. 1).

Computed tomography scan of the mass invading the rectus sheath.
In view of the uncertainty of this patient's diagnosis, surgical exploration was chosen, with the involvement of both a consultant gynecologist and a consultant surgeon. Informed consent was obtained from the patient. Operative findings showed a single 5-cm mass invading the rectus sheath. The mass was excised completely. However, due to the large defect that resulted in the rectus sheath, a small mesh was sutured to the edges of the rectus sheath to close the defect (Fig. 2).

Intraoperative view of the endometriotic mass and mesh tailored to cover the defect created by excision of the mass.
Results
The mass was sent for histopathologic examination, which showed endometriosis (Fig. 3). A postoperative follow-up at 18 months showed that this patient had an uneventful recovery.
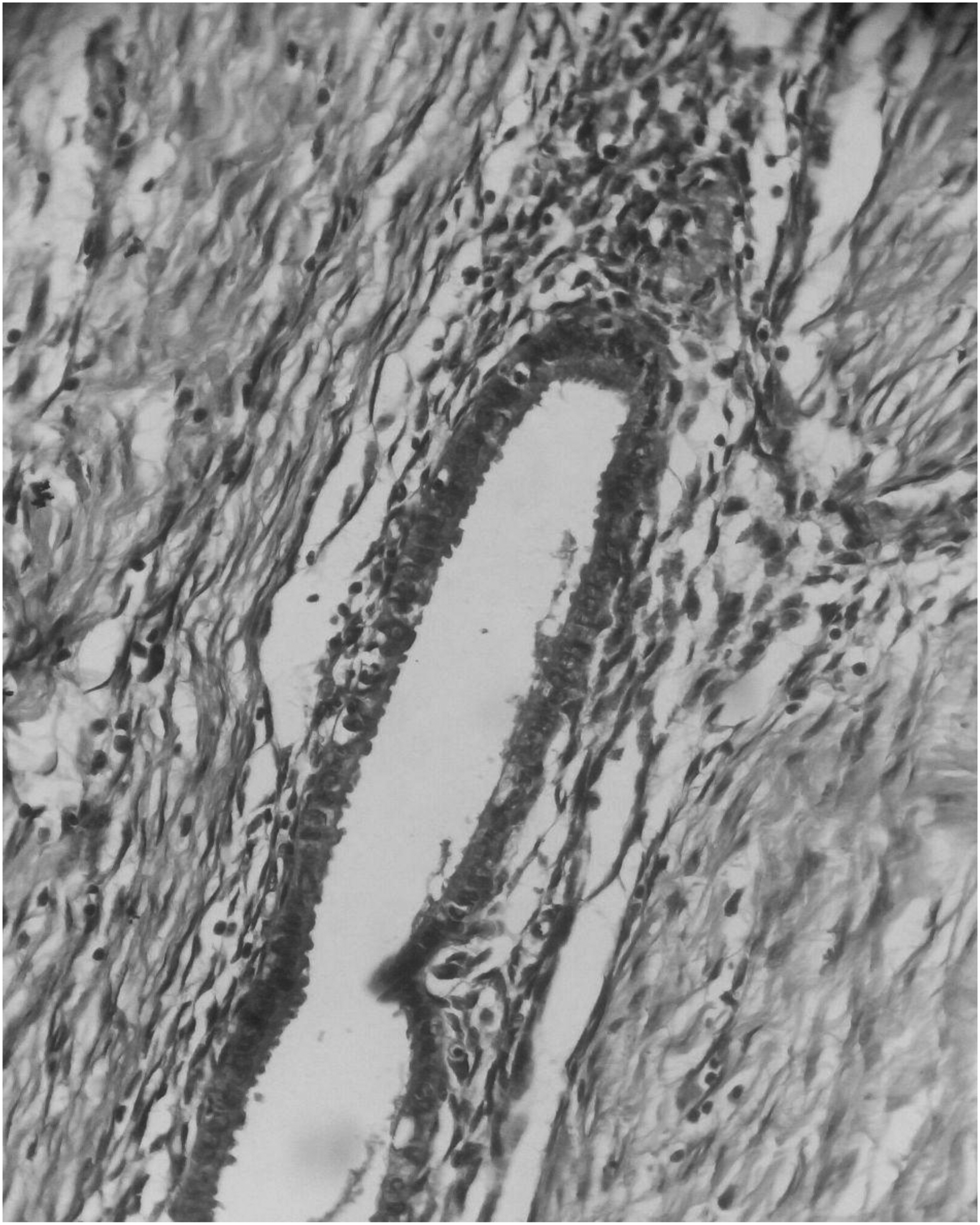
Microscopic view of the excised mass. Rectus sheath endometriosis at 400 × , hematoxylin and eosin stained.
Discussion
Scar endometriosis is a rarely reported condition present in women who have had previous pelvic or abdominal operations. 3 The incidence has been estimated to be between 0.03% and 0.15% of all cases of endometriosis.1,2 Many theories have been suggested for the cause of such a condition. The most popular theory is intraoperative transplantation of endometrial cells around the edges of wounds made during pelvic or abdominal surgeries.1,2,4,5 Another appealing theory states that endometrial implants are derived from stem cells; this was shown in an animal study by Du and Taylor, 6 who found stem cells populating endometriotic implants in hysterectomized mice, suggesting disease progression even after hysterectomy.
It is difficult to diagnose scar endometriosis. Cyclic changes in the size and degree of pain with the menstrual crescendo is characteristic of classical endometriosis. However, this is not so in most cases, especially because this phenomenon is patient-dependent. Ding and Hsu 7 reported such cyclic changes in only 20% of their patients. The current case needed the involvement of a consultant surgeon and a consultant gynecologist because the diagnosis was not established except after histopathologic examination.
Management of these cases may be by hormonal suppression or surgical excision.8,9 Hormonal suppression includes progesterone, androgen, and oral contraceptive pills. However, this approach might be only partially effective; surgical excision of the scar is the definitive treatment.9,10 In the current case, surgical excision was chosen as the primary treatment, especially because the diagnosis was not certain. This approach was similar to the management used by Badawy and coworkers 11 in 3 cases of cesarean-section scar endometriosis. However, Badawy and coworkers were sure of the diagnosis for their 3 patients, as CT scanning and needle biopsy were both used to confirm the diagnosis preoperatively.
Conclusions
Scar endometriosis is a rare and deceptive condition that might mimic incisional hernia or tumors invading the rectus sheath, thus, requiring a high level of suspicion.
Footnotes
Author Disclosure Statement
No competing financial conflicts exist.