
Abstract
Abstract
Background:
With the increasing rate of abortion and other intrauterine operations, uterine arteriovenous malformation (AVM) is no longer a rare entity. It can cause irregular uterine bleeding with subsequent anemia and even massive life-threatening uterine hemorrhage. Selective arterial embolization is often used as first-line treatment for this condition.
Case:
A 29-year-old women, gravida 5, para 1, had lower abdominal pain and intermittent vaginal bleeding. She had had one cesarean section and four artificial abortions. Thirteen days prior to presentation, she had undergone an artificial abortion via intrauterine aspiration. Ultrasound examination revealed an area of increased vascularity in her posterior uterine wall, which measured 18 mm × 15 mm × 7 mm. Hysteroscopy revealed a reddish spongy area in the posterior uterine wall. The patient was treated successfully with hysteroscopic roller ablation of the vascular mass, which was dehydrated and then separated from the uterine wall.
Results:
The patient recovered smoothly, and ultrasound examinations showed that there were no vascular masses in subsequent follow-ups.
Conclusions:
Hysteroscopic roller ablation could be a safe, feasible technique for treating AVM. However, further studies with longer-term follow-ups are needed to prove the technique's efficacy. (J GYNECOL SURG 33:37)
Introduction
U
The symptoms of AVM involve frequent vaginal spotting, irregular uterine bleeding or inadvertent massive bleeding. Conservative methods—such as multiple selective arterial embolization or transcutaneous embolization—are preferred because these patients are often in their reproductive years.2,3 Hysterectomy is mandatory in case of failure. 4 Given that intrauterine lesions are often present in cases of AVM,3,4 the current authors hypothesized that hysteroscopy could play a role in treatment for AVM. This article presents a case of AVM that was managed successfully with hysteroscopy.
Case
A 29-year-old women, gravida 5, para 1, presented at a gynecologic clinic because she had lower abdominal pain and intermittent vaginal bleeding. Her past medical history included one cesarean section and four artificial abortions. Thirteen days prior to presentation she had an artificial abortion via intrauterine aspiration. After that operation, she had intermittent vaginal bleeding. Her lower abdominal pain had started 3 days prior to admission. An ultrasound examination revealed an area of increased vascularity in her posterior uterine wall, which measured 18 mm × 15 mm × 7 mm. As shown in Figure 1, a detailed evaluation of this area with pulse Doppler showed vessels with multidirectional high-velocity flows that produced a “color mosaic” pattern. The patient was diagnosed with uterine AVM. Then she was admitted to a hospital for further treatment.
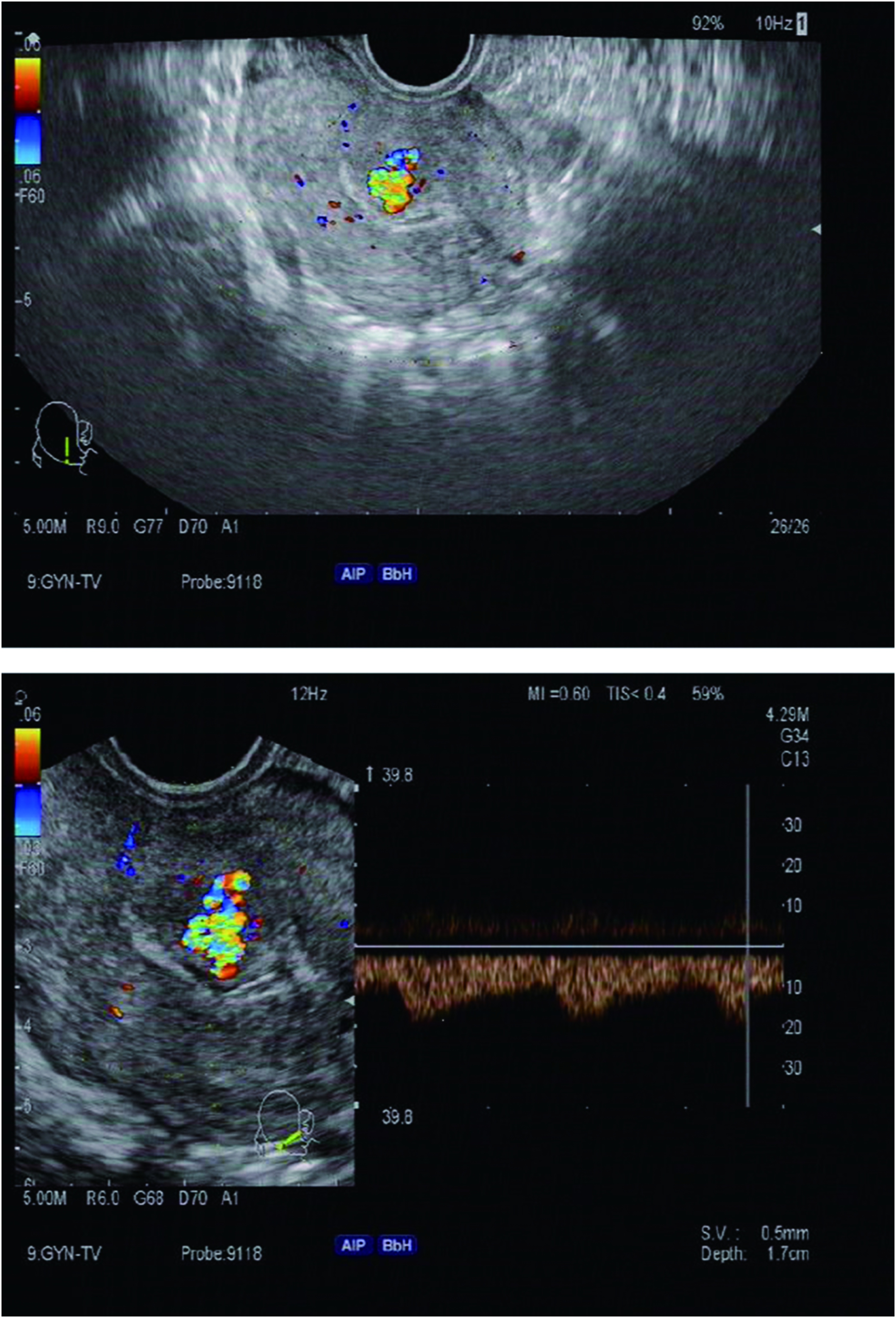
Transvaginal Doppler ultrasound images of the uterus reveal the enlarged, high flow vessel located in the posterior wall of the uterus. Color images available online at www.liebertpub.com/gyn
Gynecologic examination revealed no abnormality except the presence of blood in this patient's vagina. When she was admitted, her human chorionic gonadotropin level was 297.02 mIU/mL; this level dropped spontaneously to 191.70 mIU/mL after 2 days. As shown in Figure 2, magnetic resonance imaging (MRI; 2 images) revealed a 15 mm × 13 mm vascular mass in the posterior uterine wall. The signal was uneven, and the boundary was unclear. There was no clear margin between the mass and the endometrium. The mass was unevenly enhanced after intravenous contrast administration. The diagnosis of uterine AVM was considered again. After careful patient consultation and preoperative preparation, hysteroscopy was chosen to address the AVM. Informed consent for the operation was obtained from the patient preoperatively. The operation was performed by the first author (Q.W.).
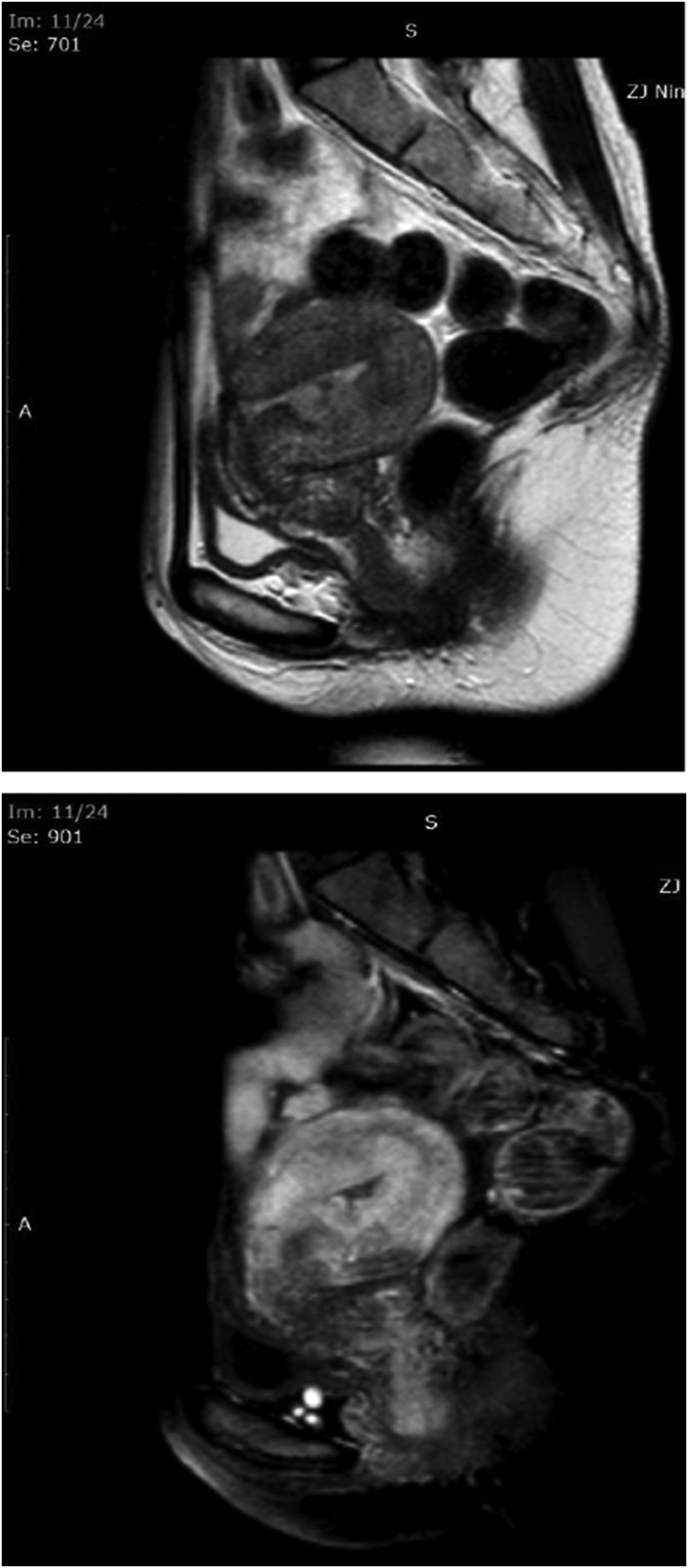
Magnetic resonance images of the arteriovenous malformation show the lesion in the posterior wall of the uterus.
Hysteroscopy was performed under general anesthesia using a 30° hysteroresectoscope (27050SL, Karl Storz, Tuttlingen, Germany). An electrolyte-free solution containing 5% glucose was used as the distending medium. An inflow pressure of 100 mm Hg was maintained by an automatic fluid pump.
Misoprostol (400 μg; Cytotec,® NPILPharmaceuticals Ltd., United Kingdom) was administered vaginally 3 hours before surgery. After the cervix was dilated with a Hegar dilator up to size 9, the resectoscope was inserted into the uterine cavity under direct vision through a video camera. Hysteroscopy showed that the uterine cavity had a normal appearance except for the presence of a reddish spongy area in the posterior uterine wall, as shown in Figure 3. Because of this area's rich vascularity, a roller electrode was chosen, instead of a loop electrode, to dehydrate the mass (Fig. 4). The electrosurgical generator was set at 110 W for cutting and at 70 W for coagulation. However, only the coagulation mode was used. Transabdominal ultrasonographic monitoring was used to ensue the safety of the operation.

Hysteroscopic view of the lesion. Color images available online at www.liebertpub.com/gyn
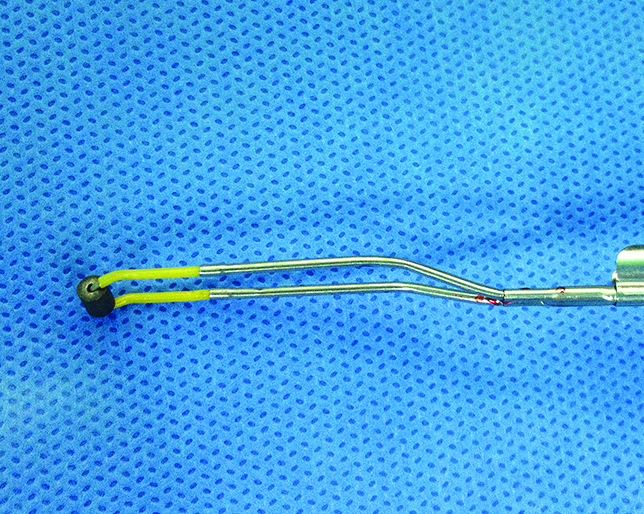
The roller electrode. Color images available online at www.liebertpub.com/gyn
Preparations for laparoscopy were also made in case of an emergency. The principle of compressing from a peripheral area to a central area was followed. The vascular mass became smaller gradually, and then was totally dehydrated and detached from the uterine wall. The total operating time was 35 minutes, and the fluid deficits were ∼810 mL.
Results
After the operation, a Doppler ultrasound scan showed that there was no vascular mass in the posterior uterine wall. Pathologic testing of an excised specimen revealed hyperproliferation of vessels and severe physical damage of the tissue.
There were no complications following the procedure, and the patient was discharged after 3 days. At her 1 month follow-up, an ultrasound scan showed complete disappearance of the AVM. Her normal menstruation was restored 30 days postoperatively. No reoccurrence was reported during her 3-month follow-up.
This patient's consent for this case report was obtained after the operation. The local institutional review board also approved this report.
Discussion
AVM of the uterus is a high-pressure, high-flow system with blood coursing through to the venous system and bypassing the capillary vessels. The venous system is in a high-pressure and a high-flow state, resulting in an increased propensity toward bleeding. In ultrasound examinations AVMs appear as heterogeneous, hypoechoic, indistinct tubular or cystic areas of variable sizes. Color Doppler scanning shows tortuous vascular structures, with multidirectional flows.
AVM cure could be achieved if this hypervascular mass was devascularized or removed. This forms the theoretical basis of various current treatments. Selective uterine artery embolization is a proven safe and effective treatment method for AVM. Published articles about uterine AVMs treated with embolization have reported success rates of 71%–93%.5–7 However, up to 32% of patients required multiple arterial embolizations.5–7 What is more, patients who undergo embolization are exposed to significant doses of radiation as well as the risk of compromised ovarian function.
The current authors considered hysteroscopy as another feasible method for addressing selected cases of AVM. The main risk of hysteroscopy is excessive bleeding, which may obscure the view and prevent a surgeon from proceeding further with the operation. An attempt was made to avoid this unfavorable condition by adopting the following two measures: (1) A roller electrode was chosen because it provides a large contact area, minimizing the risk of cutting into the vessels. (2) the flow of blood in the vessel could carry away the heat from the electrode rapidly, so the principle of compression from peripheral to central areas was followed. After constriction and atresia of vessels in the peripheral area, the roller was carried to the central area, then the whole vessels were dehydrated.
Fertility after these procedures remains speculative. No specific fertility data are currently available. However, hysteroscopic management is probably better than other methods for preserving subsequent fertility because of less inference with the uterine vessel system. Conversion to laparoscopy or embolization can be implemented immediately in cases of failure.
Conclusions
Uterine AVM can be managed by hysteroscopy in selected cases. The technique of roller ablation was a safe, feasible technique for treating a patient's AVM in this case. However, the efficacy of this method in more-advanced cases is not yet clear. More studies with longer-term follow-ups are needed to prove this technique's efficacy.
Footnotes
Acknowledgment
The current authors thank the patient who donated her medical data to make this contribution to scientific research.
Author Disclosure Statement
The authors have no potential conflicts of interest to disclose.