
Abstract
Abstract
Introduction
P
Case
A 25-year-old woman was admitted to Safdarjung Hospital, in New Delhi, India, with a cystic mass in the retrorectal region. She was operated on to treat dysgerminoma of her right ovary, followed by a hysterectomy and bilateral salpingo-oophorectomy. Magnetic resonance imaging (MRI) revealed a 23 × 21 mm cystic lesion that was hyperintense on T2 and hypointense on T1. It was located posterior to her rectum, closely abutting the rectal wall (Fig. 1). A small tract was also seen extending inferior to right levator and up to the intersphincteric plane on the right side. However, no bony communication was seen. A total mass excision of the lesion was performed and sent for histopathologic examination. Gross examination revealed that the specimen was a gray–brown piece of soft tissue measuring 3 × 2.5 × 2 cm.

Magnetic resonance imaging showed a 23 × 21–mm cystic lesion located posterior to the rectum, closely abutting the rectal wall.
Results
Histopathology testing of the specimen showed features of an epidermoid cyst (Fig. 2). The patient has been on follow-up since 1 year and has been doing well.
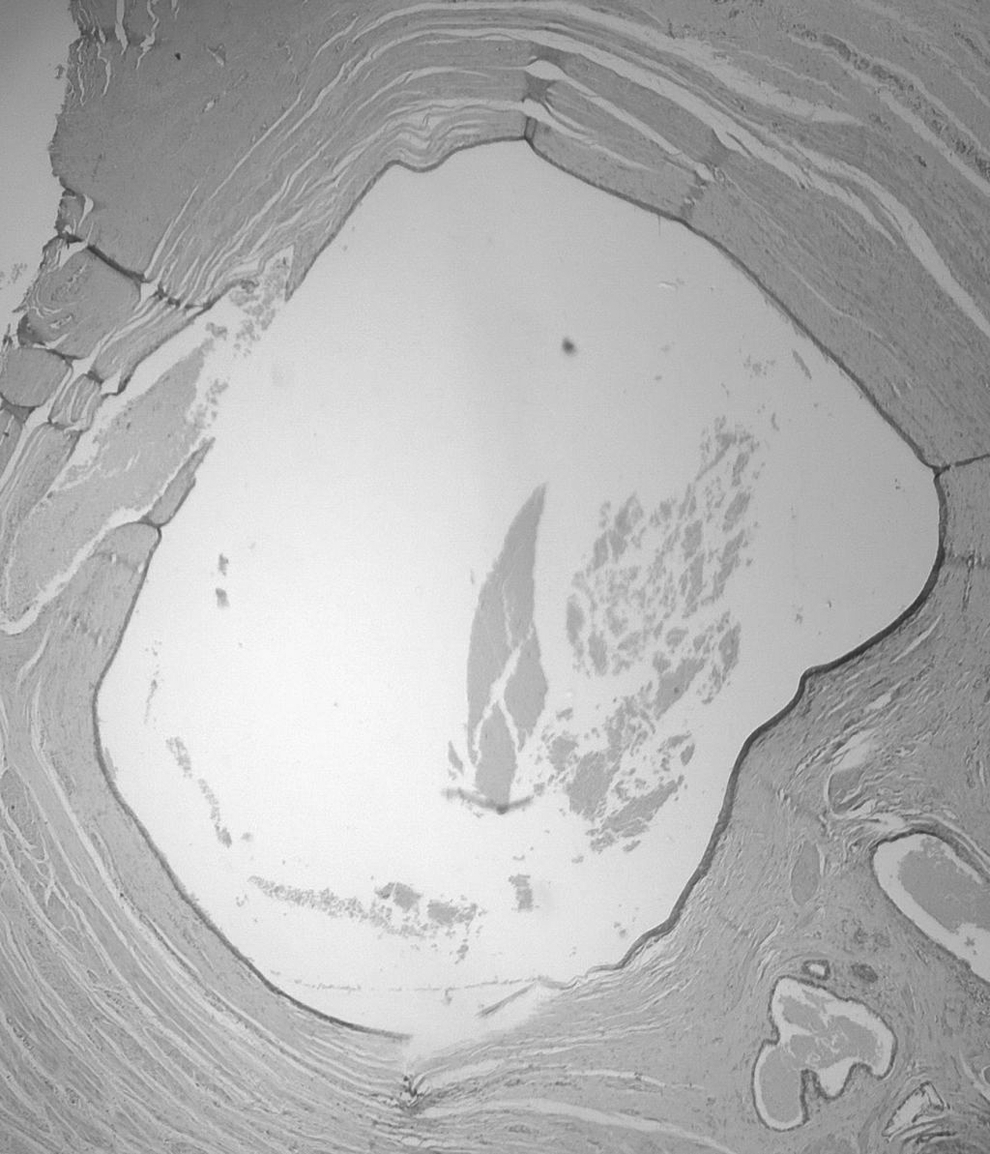
Histopathologic examination showed epidermoid cysts lined by stratified squamous cells devoid of skin appendages (hematoxylin and eosin, × 40).
Discussion
A large series from the Mayo clinic reported a 1 in 40,000 incidence of retrorectal tumors. 4 The majority of retrorectal tumors are benign. These tumors are broadly categorized as inflammatory, congenital, neurogenic, osseous, and miscellaneous. 5 Congenital lesions account for >50% of all retrorectal tumors and approximately two-thirds of them are developmental cysts. These include epidermoid, dermoid, enteric, tailgut (also known as retrorectal cystic hamartomas), and duplication cysts. Developmental cysts are usually seen during childhood, and they are relatively rare in adults. 3
The majority of developmental cysts are asymptomatic, as they occupy the hollow of the sacrum and are missed even on rectal examination because low tension in the cysts. 6 When present, symptoms are related to the mass having an effect caused by local compression on the rectum and lower urinary tract that leads to constipation, rectal fullness, painful defecation, lower abdominal pain, dysuria, and urinary frequency. The most important complications of developmental cysts are infection and fistula formation; 30%–50% of developmental cysts are complicated by chronic infections. When infected, the cyst can present with a sinus communicating with the exterior and can often raise the differential of a pilonidal sinus or even an anal fistula. Bleeding related to ectopic gastric mucosa or mucosal irritation is rare, as is malignant degeneration.6,7
On computed tomography scanning, an epidermoid cyst will appear as a well-defined oval that has a thin-walled unilocular formation with low attenuation. Rarely, an epidermoid cyst can be associated with fine calcifications. 3 If the cyst is infected, the walls may appear thickened with pericystic inflammatory changes. Typically, developmental cysts are hypointense on T1-weighted MRI scans. The presence of mucoid material can result in hyperintensity. Focal irregular wall thickening with enhancement is suggestive of malignant degeneration.3,6,7 Endorectal ultrasonography can also be performed, as it helps with assessing rectal-wall involvement and pelvic-floor muscle invasion. 6
Epidermoid and dermoid cysts are the direct result of closure failure of the ectodermal tube. Histopathology testing shows that epidermoid cysts are composed of stratified squamous cells and are typically benign unilocular lesions that do not contain skin appendages. Unlike epidermoid cysts, dermoid cysts have stratified squamous epithelia with skin appendages (e.g., sweat glands, hair follicles, sebaceous cysts). 8 Other differential diagnoses at this site include sacrococcygeal teratomas, which can be ruled out on the basis of age; and meningoceles, which can be ruled out because of absence of bony defects and lymphangiomas, the histopathology of which would reveal dilated lymphatic spaces. 7
Conclusions
As epidermoid cysts are rare in adults, they often pose diagnostic and therapeutic challenges.
Treatment involves complete excision of the cyst and the sinus, because of the risk of recurrence, malignant degeneration, and chronic infection. 1 As these lesions are frequently adherent to the coccyx, en bloc coccygectomy is preferred for larger lesions.6,7
Footnotes
Author Disclosure Statement
No financial conflicts exist.