
Abstract
Abstract
Objectives:
There were two objectives: (1) to assess the survival outcome of endometrial cancer based on surgical and adjuvant treatment and (2) to note patterns of and risk factors for recurrence in endometrial cancer.
Design:
This was a retrospective analysis of the hospital records of women diagnosed with carcinoma of the endometrium who were operated on in the Division of Gynecologic Oncology, Christian Medical College, Vellore, India, from January 2011 to December 2013.
Materials and Methods:
Electronic patient records of 152 women with endometrioid endometrial cancer were obtained and used to analyze their surgical outcomes. Information regarding survival and recurrences was obtained by various methods. Survival was assessed by Kaplan–Meir survival analysis.
Results:
The tumors were endometrioid adenocarcinomas in 94.7% of the patients. The majority of the patients were stage IA (49.3%) and stage IB (22.3%). A few patients also had occult stage II (6.6%), and 21% had advanced stage cancer. Seventy-seven (50.7%) women needed adjuvant treatment after risk stratification, with 53.6% receiving radiation only as brachytherapy (35.6%), external pelvic radiation (13.5%), or a combination of both (50.9%); 15.9% received chemotherapy; and 30.4% had radiation and chemotherapy. The 3-year survival of endometrial cancers was 94.5% and disease-free survival was 91.4%. The rate for recurrence was 8.6% and for mortality 5.5%. Recurrences were equal in distribution for local and distant metastasis. Complications of surgical treatment were minimal.
Conclusions:
Endometrial cancers tend to present as early stage cancers in the majority of cases. Appropriate risk stratification and liberal use of chemotherapy when indicated may improve survival in high-risk cases. (J GYNECOL SURG 2017:1)
Introduction
E
The International Federation of Gynecology and Obstetrics (FIGO) staging of endometrial cancer and other gynecologic cancers was revised in 2009.4,5 The Gynecologic Oncology Group (GOG) 99 trial reported different survival in different risk groups based on various prognostic factors such as age, myometrial invasion, grade of tumor, and lymph-vascular space invasion. 6 In the current authors' institution (Christian Medical College, Vellore, India; CMC) gynecologic oncology became a super-specialty since 2011. Ever since that time, there has been strict adherence to guidelines, and comprehensive cancer surgeries are being performed. This study was undertaken to assess the surgical outcomes of endometrial cancer, the patterns and risk factors of recurrence in endometrial cancer, and to determine the complications of surgical treatment in a tertiary institution such the CMC.
Materials and Methods
Patients in the analysis
Patients diagnosed with carcinoma of the endometrium, who underwent surgical staging, from January 1, 2011, to December 31, 2013, were recruited in the study after ethical clearance from the CMC's institutional review board. Data regarding baseline characteristics, disease profiles, surgical outcomes, complications, biopsy details, and adjuvant treatment details were collected from the electronic records and supplemented with patients' letters and phone interviews. All endometrial cancers, operated on in the Gynaecologic Oncology Division of the CMC were included. Patients who underwent incomplete surgery elsewhere and came to the CMC for completion procedures, and whose initial operative details were not available, were excluded.
Outcome measures
Outcome measures included the use of blood and blood products, and complications of surgery, such as infections, hemorrhage, wound breakdown, and lymphocysts. Recurrence was diagnosed based on clinical and radiologic imaging. A local recurrence was defined as any disease confirmed by histopathologic examination at the vault region. Distant recurrence was defined as disease out of the pelvis as shown clinically or on imaging.
Disease-free survival (DFS) was defined as the period during which a patient was free of local or distant disease clinically and radiologically. Overall survival was assessed over 36 months. These survival data were correlated to disease stratification, adjuvant treatment, and prognostic factors.
Staging and procedures in the analysis
At the CMC, all patients were staged according to the 2009 FIGO criteria. The protocol followed for lymphadenectomy was a slight modification of the guidelines for surgical management of endometrial cancer from the Mayo Clinic.7,8
As the CMC did not have a facility for examining intraoperative frozen sections, a decision for assessing tumor volume was based on naked-eye examination when cutting open a specimen.
Pelvic lymph-node dissection involved opening of the retroperitoneum and removing all fibrofatty tissues along the major pelvic vessels. The distal limit of the node dissection was up to the circumflex iliac vessels over the external iliac and the obturator nerve, leaving the pelvis at the obturator fossa. The upper limit was the common iliac nodes at the bifurcation of the common iliac arteries.
Para aortic-node dissection was performed up to the level of the inferior mesenteric artery.
Completion surgery (post hysterectomy) for patients operated on elsewhere was offered if there was deep myometrial invasion, or a grade 3 tumor, or if high-risk histology and ovaries had been retained. Baseline imaging was performed, followed by a restaging laparotomy that included peritoneal washings, and pelvic and para-aortic-node dissection as indicated.
Adjuvant treatment was offered per institutional guidelines following a discussion at a multidisciplinary meeting (Appendix 1). These guidelines were formulated per the National Comprehensive Cancer Network guidelines.
Patients were followed up once every 3 months for the first 2 years, then once every 6 months for 5 years.
Statistics
The data were analyzed using SPSS software (version 19). Statistical tests performed were the χ2 test, Fisher's exact test, and Kaplan-Meier survival analysis. The degree of significance was set at p < 0.05. Linear regression was used to study the determinants of survival and recurrence.
Results
During the study period, a total of 162 women were operated on for endometrial cancer. Ten women whose operative details were not available were excluded from the study. The average age was 56 (range: 30–79) and the mean body mass index was 28.7 (range: 15.9–46). The majority of the patients presented with postmenopausal bleeding (77%). Premenopausal abnormal uterine bleeding and anovulatory cycles with metropathia were the other presenting complaints. Histories of infertility were noted in ∼13.2% of the patients. Medical comorbidities were seen in 71.9% of the patients, as most of them were older (Table 1). Histories of treatment for breast cancer and treatment with tamoxifen were seen in 11 (7%) women.
BMI, body mass index; AUB, abnormal uterine bleeding; IU, international units; TVS, transvaginal ultrasound.
In this series, the preoperative histology was endometrioid in 94.7%, and most were grade 1 tumors (72.2%). Postoperative biopsies revealed endometrioid histology in 88.8% and grade 1 differentiation in 57.9%.
Most of the women underwent complete surgical staging as indicated by the institutional protocol. A few of them (15 [9.9%]) had undergone simple hysterectomy as they had had early stage (< IA) disease. Thirteen of them had undergone other procedures, which included completion surgeries (10) and radical hysterectomies (3) (Table 2).
TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; PLND, pelvic lymph-node dissection; PAND, para-aortic node dissection; LAVH, laparoscopic vaginal hysterectomy; VH, vaginal hysterectomy.
Pelvic lymphadenectomy, as indicated by the CMC institutional protocol, was performed in 126 of the 152 patients, with a mean count of 13 nodes. Sixteen (13%) of these patients had pelvic-node metastatic disease. Thirty-two patients underwent para-aortic node dissection, with an average node count of 10 with metastasis in 8 (28%). Omentectomy was performed in 29 (19%) of the patients when indicated. In some patients with serious comorbidities, laparoscopic hysterectomy or vaginal hysterectomy was performed. More than 80% of the series patients underwent surgical staging by a midline incision under general anesthesia and epidural anesthesia (73.3%).
Considering the fact that majority of the patients underwent surgical staging by laparotomy involving a longer operating time and large incisions, as well as the prevalence of a high incidence of diabetes, the complication rate in this series was ∼28% (43/152 patients; Table 3).
DVT, deep vein thrombosis; ICU, intensive care unit, HDU, high-dependency unit.
Approximately two-thirds of the tumors were >2 cm (67.1%) and predominantly endometrioid (88.2%). In a few patients, the tumors were high grade (12.5%). The nonendometrioid tumors were 11.8% comprising serous (4), clear-cell (1) and mixed (3) type tumors. Lymph-vascular space invasion (LSVI) was seen in 41 (27.0%) patients, with deep myometrial invasion in 56 (36.8%) of them (Table 4).
LVSI, lymph-vascular space invasion; PLND, pelvic lymph-node dissection; PAND, para-aortic node dissection.
The majority of the patients in this series had stage IA and stage IB (71.7%) disease. A few of these patients also had occult stage II (6.6%) disease. Approximately 21% had an advanced stage of disease beyond stage III (Table 5).
The final histopathology of these patients was discussed at a multidisciplinary team meeting, and decisions on adjuvant treatment were made. Of the 75 (49.3%) patients with stage IA disease in this study group, 73 patients had grade 1 or 2 tumors and, hence, did not receive adjuvant treatment (Table 6). Of the remaining 77 patients who needed adjuvant treatment, 69 (90%) underwent adjuvant treatment in some form. Thirty-seven had only radiation, 11 had only chemotherapy, and 22 had a combination of both chemotherapy and radiation. Of the 59 (86%) patients who underwent radiation in some form, vaginal brachytherapy alone was administered in 21 patients, pelvic radiation in 8, and a combination of both in 30. Vaginal brachytherapy was delivered at ∼1-month postsurgery, using a vaginal mold to help deliver high dose-rate fractions of 6–8 Gy. Pelvic radiation was either by conventional or intensity-modulated radiation therapy of 50 Gy in 25 fractions. In more than half (30/59) of the patients, a combination of pelvic radiation followed by vaginal radiation was administered.
In some patients, when indicated, chemotherapy was offered as adjuvant therapy (33). Four cycles of a combination of paclitaxel and carboplatin were given after sutures were removed in more than two-thirds of patients who received chemotherapy. In a few situations when there was taxane sensitivity, single-agent platinum drugs were chosen.
Adjuvant treatment was assessed by risk stratification in the treatment of the endometrioid tumors (135). Eighty-three women were found to be in the low/low–intermediate risk group, 25 in the high–intermediate risk group, and 27 in the high-risk group. The adjuvant treatment of these groups is shown in Table 7. A few of these women were also offered chemotherapy in addition to the radiation, especially when they had high-risk features such as positive peritoneal cytology, LVSI, and node positivity.
EBRT, external beam radiation therapy; IR, intermediate risk.
There were 15 recurrences (Table 8) overall with disease-free survival of 4–48 months and recurrence rates of 9.8%. Five recurrences were in the nonendometrioid group (17), whereas there were 10 (7.4%) recurrences in the endometrioid (135) tumor group (Figs. 1–4). Eight of the 10 recurrences in the endometrioid group were stage IB where there was deep myometrial invasion. Metastasis was a combination of distant and local in 12 of the patients, whereas 3 patients had only distant recurrences. The sites of recurrences were predominantly in the para-aortic nodes (12), abdomen (3), omentum and inguinal nodes (1), and umbilical nodule (1). Eight patients succumbed to the disease over the follow-up period of 36 months, with an overall survival of 94.7% (Table 8).
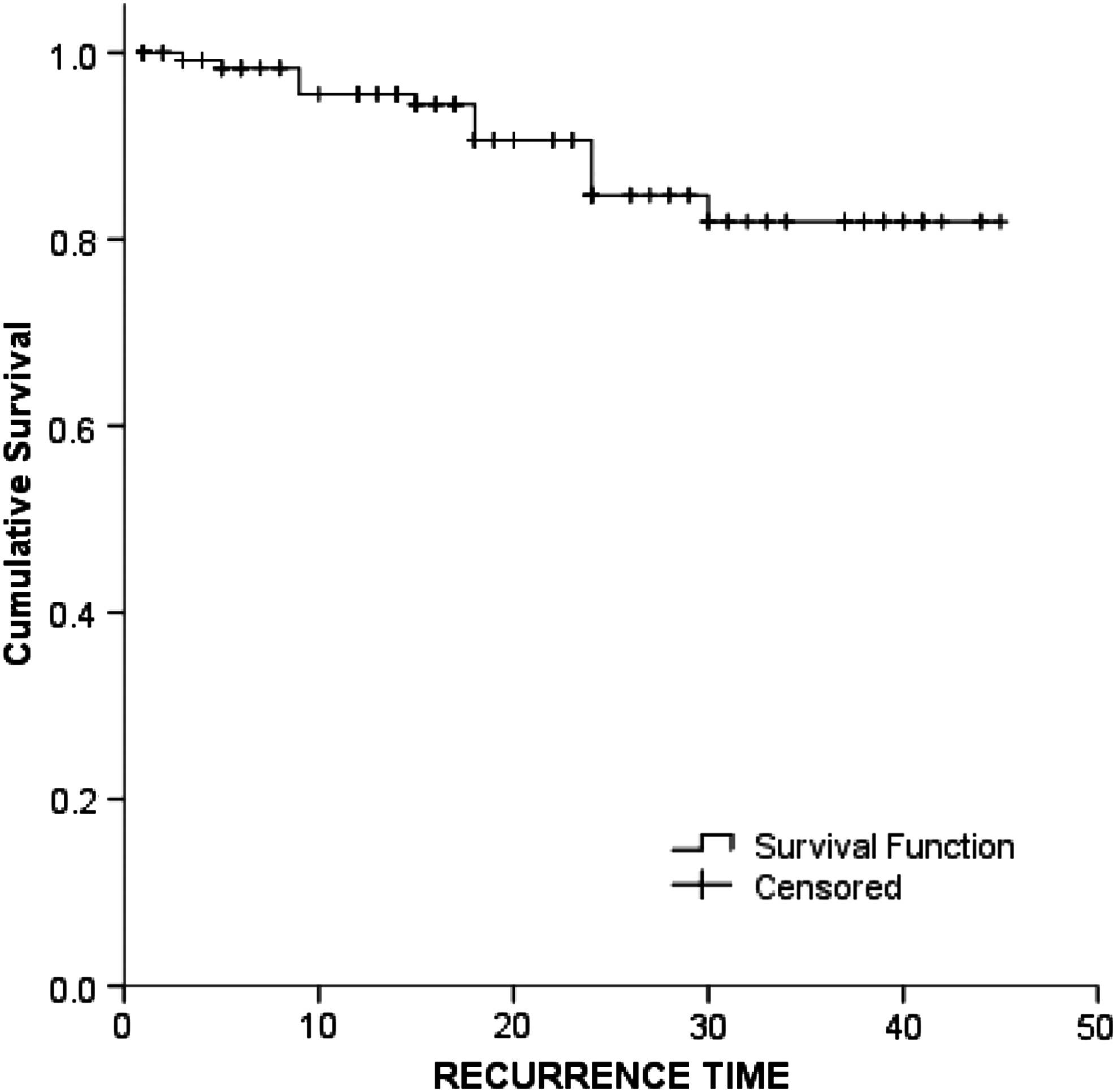
Disease free survival—91.4%.
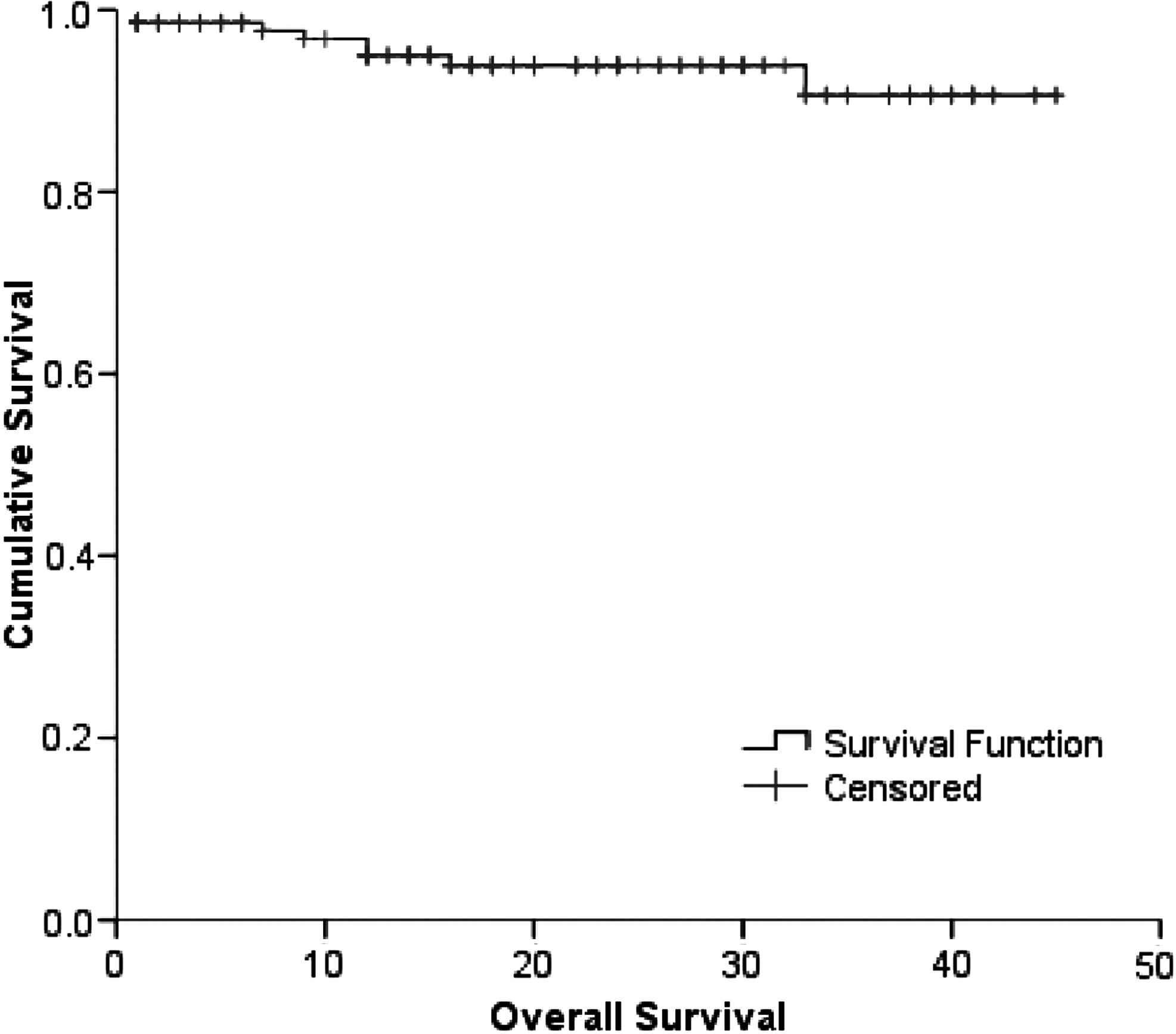
Overall survival—94.7%.
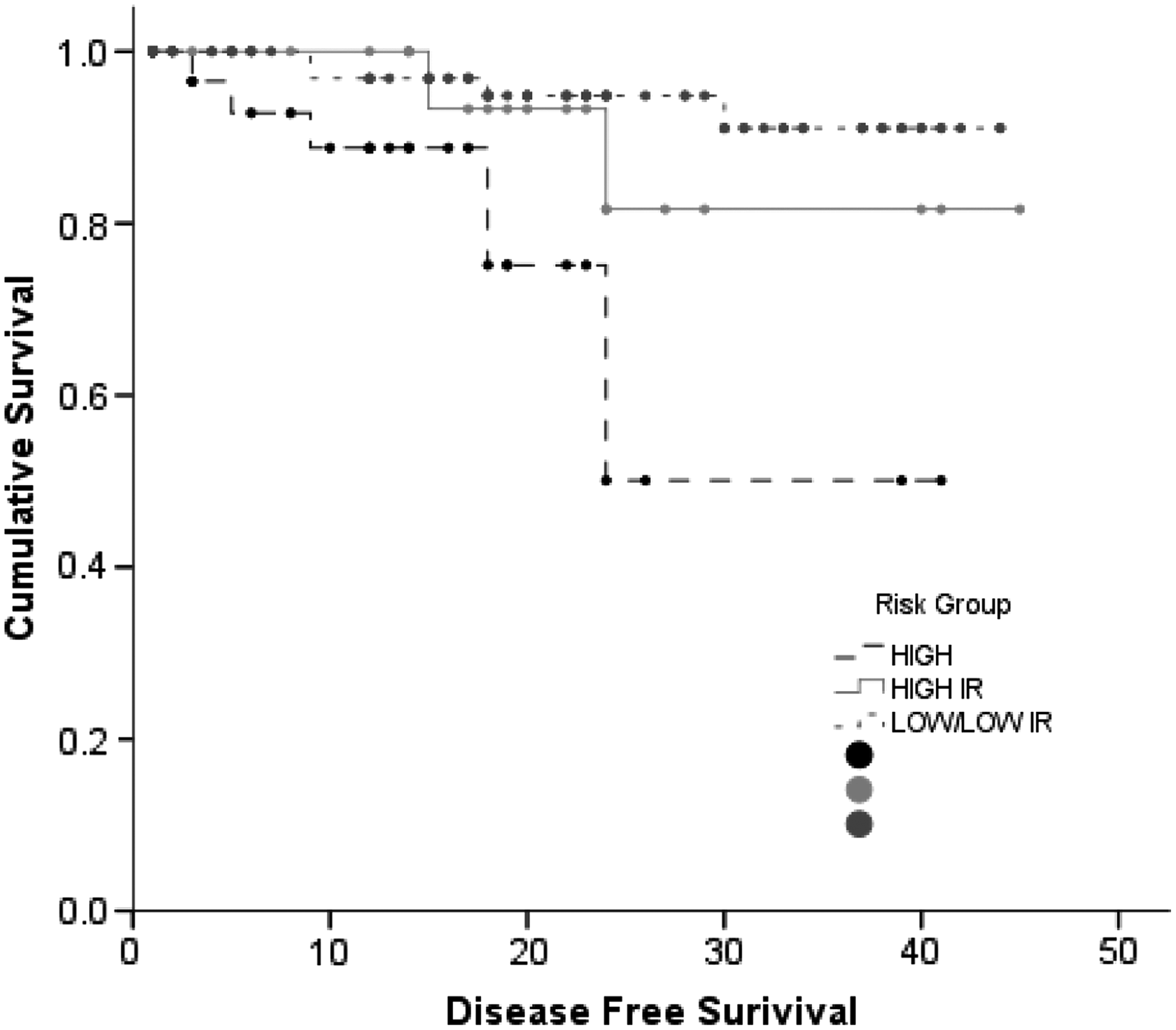
Disease-free survival in endometrioid endometrial cancer.
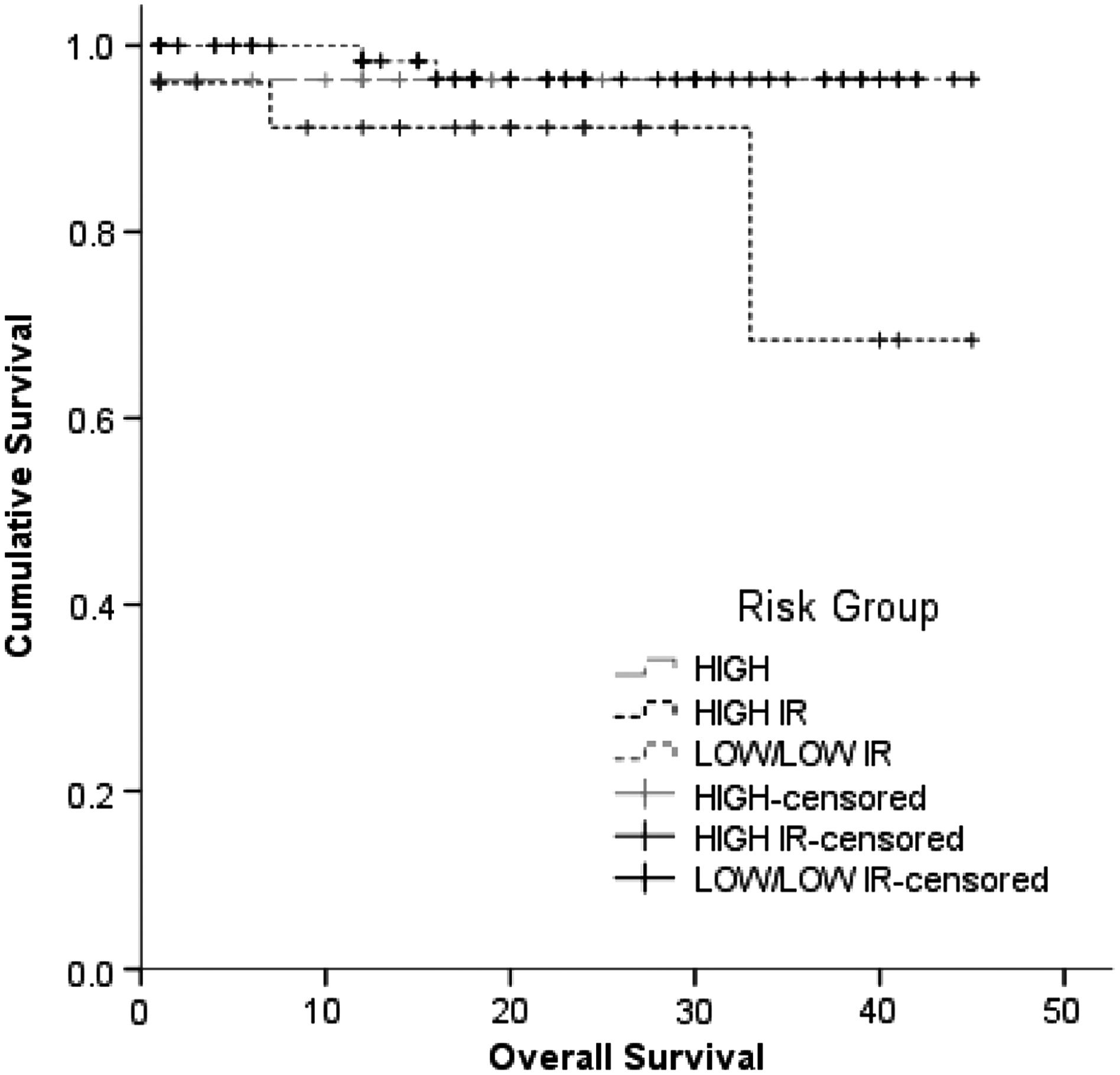
Overall survival in endometrioid endometrial cancer.
An attempt was made to examine various factors that could have possibly affected survival (Table 9). A logistic regression was computed for all of these factors. Risk factors of deep myometrial invasion, higher grade of tumor (G3), parametrium being positive, and adjuvant treatment were significant for DFS on univariate analysis. However, an adjusted analysis was not statistically significant for these factors. Similarly, for overall survival, only infertility and higher grade of tumor (G3) were significant on univariate, and no factors were significant after adjusting for each other on multivariate analysis.
(R) in Table 9 denotes the least risk.
OR, odds ratio; CI: confidence interval, LVSI, lymph-vascular space invasion.
Discussion
Endometrial cancer is one of three commonly occurring gynecologic malignancies. On average these cancers comprise ∼30%–40% of gynecologic cancers that are operated at the CMC. The retrospective analysis of surgical outcomes from this tertiary hospital emphasizes the importance of comprehensive surgical staging and adherence to protocols based on which treatments need to be carried out to result in better outcomes. Endometrial cancer is a disease that occurs primarily in postmenopausal women, and the prognosis worsens with advancing age, as the nature of disease changes in that age group. The role of estrogen in the development of most endometrial cancers has been established clearly. Any factor that increases exposure to unopposed estrogen increases the risk for endometrial cancer. With the rise in the rates of the obesity epidemic, an increasing number of younger girls tend to develop anovulatory cycles, leading to longer durations and higher incidences of estrogen exposure. In the study group of 152 patients, there were ∼10 women under age 40. Most of these women had histories of anovulation and infertility, and the number of affected patients is increasing. Patients having tamoxifen prophylaxis for carcinoma of the breast need adequate surveillance. Histories of treatment for breast cancer and treatment with tamoxifen were seen in 11 (7%) of the study women.
Preoperative evaluation for the grade, size of tumor, and extent of disease is important in guiding surgeons to decide the extent of surgery. Ultrasound examination was performed routinely for all of the study patients, per the CMC institutional protocol. The surgeries were all performed by the surgeons in the CMC's Gynaecologic Oncology Division, who had adequate training in comprehensive surgery and lymphadenectomy.
Surgery for endometrial cancer has undergone significant advances. Many studies have proven that the minimally invasive route of surgery, whether laparoscopic or robotic, has a favorable outcome with regard to survival, lymph nodes, and fewer complications. The only drawbacks of minimally invasive surgeries are the costs involved and the operating times. 9 A Cochrane meta-analysis recently concluded that there is evidence to support the role of laparoscopy for the management of early endometrial cancer. For presumed early stage primary endometrioid adenocarcinoma of the endometrium, laparoscopy was associated with similar overall and DFS. Laparoscopy was associated with reduced operative morbidity and hospital stay. There was no significant difference in severe postoperative morbidity between the two modalities. 10 In countries like ours, where gynecologic oncology as a specialty is in its early phase of development, comprehensive open surgery with appropriate and adequate lymphadenectomy, when indicated, is the need of the current time.
In this group of study, patients' open surgery was performed in >95% of the cases. Pelvic and para-aortic dissection was performed, based on per operative characteristics of the tumors.
Complications of the open procedure and lymphadenectomy were commonly occurring problems and were similar to statistics quoted by other researchers. 11 The most common serious complications were postoperative ileus and delayed bowel recovery. The other serious adverse events, such as vascular, bowel, and bladder injuries, occurred in smaller numbers.
Following risk stratification for adjuvant therapy enabled many of the patients to receive the appropriate adjuvant therapy as indicated. The current authors did observe, from this retrospective analysis, that some women in the low/low–intermediate risk group received adjuvant treatment mainly in settings where they had single high-risk features such as LVSI or high-grade tumors. Several studies conducted elsewhere in other populations showed that use of chemotherapy lowered the risk of distant metastasis but did not improve overall survival in the study populations.12–14 Despite these results, chemotherapy in patients with any high-risk factors—even those that fell into the intermediate risk group—was routinely practiced in the CMC—and this stood out as a single significant protective factor for prevention of recurrences (p < 0.001) and better survival (p < 0.04). In this series, as in the abovementioned studies, the recurrences were predominantly at distant locations especially in the nodes. Even in the low intermediate–risk group whom did not receive chemotherapy, there were local as well as distant recurrences, despite receiving pelvic radiation and vaginal brachytherapy.
With the advent of newer radiation techniques resulting in better delivery of doses to tumors and unaddressed para-aortic nodes, recurrences could be reduced. Some researchers are also evaluating the possibility of chemoradiation, as is performed for patients with cervical cancer, and its role in improving overall survival. The biology of a tumor, its behavioral pattern, and the outcome may vary with race and ethnicity; thus, suggesting the concepts of genetics, unique molecular markers, and personalized medicine.
The limitations of this study were that it was a retrospective study and some follow-up details were not obtainable. The follow-up of patients and their compliance with further treatments were not satisfactory. It is probable that the results could have been different if the follow-up had been extended up to 5 years.
Conclusions
Comprehensive surgery involving pelvic lymph nodes and para-aortic node dissection where indicated, followed by adequate adjuvant therapy, can result in better survival in early stage endometrioid cancer. Open surgery, if performed by trained surgeons, could result in outcomes as good as minimally invasive surgery in settings where facilities are not available for laparoscopy or robotics. The focus should be on adequate training in surgical skills in such situations and referral to gynecologic oncology set-ups.
Footnotes
Acknowledgments
The authors acknowledge the services of Ms. Elizabeth L. Gracy, MA, the social worker in the team who helped establish contact with the patients. Thanks are also extended to the Christian Medical College for permitting this study.
This study was funded by an internal institutional grant (IRB 8726 dated 06/03/14).
Author Disclosure Statement
None of the authors has any financial interests or conflicts in connection with this article.
Appendix 1. Surgical Protocols
| Stage I A, G1 / G2, No risk factors | Observe |
| Stage I A G3, No risk factors | VBT * |
| Stage I A (Inv <50%), Any grade, risk factors | |
| Stage I B, Any grade, No risk factors | |
| Stage I B G1/G2, Risk factors | |
| Stage II G1/G2 | VBT * + Pelvic RT ** |
| Stage I B G3, Risk factors | VBT * + Chemo + Pelvic RT ** |
| Stage II G3 | |
| Stage III, IV |
VBT, vaginal brachytherapy
Pelvic RT, radiotherapy