
Abstract
Abstract
Background:
An uncommon finding is the presence of multinucleated cells in the squamous epithelium of the vulva, unrelated to human papillomavirus (HPV) infection. Most likely a result of inflammation, these cells have been seen within the basal-to-middle layers of the squamous epithelium. This finding can be mistaken for evidence of HPV infection.
Case:
This article describes the case of a woman in her 30s who presented with chronic vulvar pruritus and whose condition remained unresponsive to multiple rounds of anticandidal therapy.
Results:
Vulvar biopsy showed multinucleated atypia in a setting of squamous-cell hyperplasia (lichen simplex chronicus).
Conclusions:
A pitfall to avoid is classifying these multinucleated cells as evidence of HPV infection. (J GYNECOL SURG 33:41)
Introduction
A
Case
A woman in her 30s with a long history of vulvar pruritus unresponsive to multiple rounds of anticandidal therapy underwent vulvar biopsy.
Results
Histology revealed hyperkeratosis, parakeratosis, and acanthosis, with mild chronic inflammation, consistent with squamous-cell hyperplasia (lichen simplex chronicus). In addition, multinucleated cells were seen in the lower portion of the squamous epithelium. There was no nuclear atypia, and these cells were not felt to represent koilocytes (Fig. 1). Ki-67 was confined to the basal layers, consistent with nonneoplastic squamous epithelium. A P16 immunostain was negative, mitigating against HPV infection. A Grocott methenamine silver stain for fungal organisms was negative.
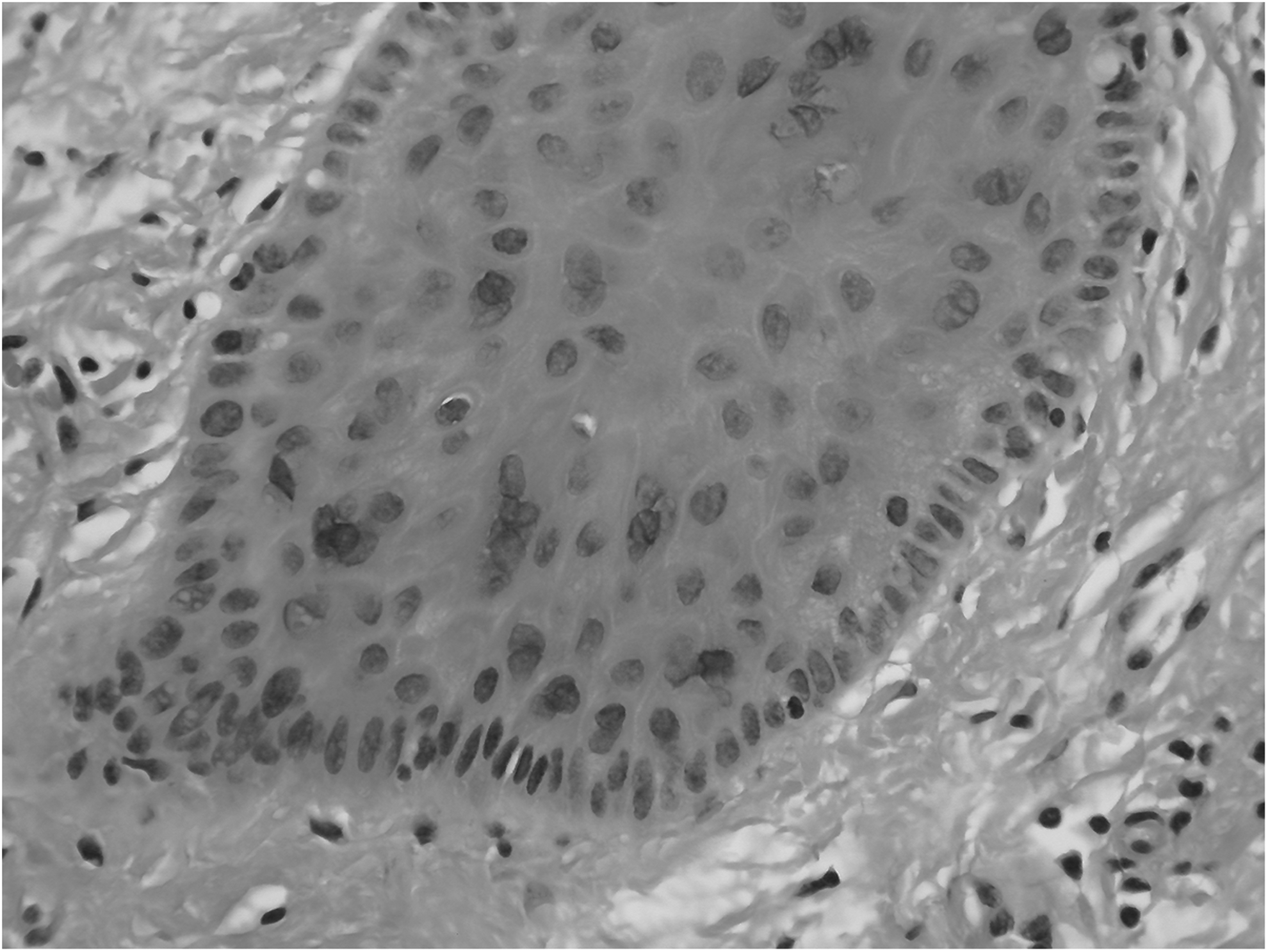
Multinucleated atypia, showing numerous multinucleated cells, with no perinuclear halos, nuclear atypia, or inflammation.
Discussion
Multinucleated atypia can occur in the basal-to-mid–epithelial layers of the mucosa of the vulva. 1 Although no specific attributable gross lesion has been established, in 1 case papules were detected, 2 possibly irritant in nature. Multinucleated atypia is usually focal and can range from single multinucleated cells to clusters of several multinucleated cells. 1 The nuclei are not atypical but may have prominent nucleoli. Perinuclear clearing may be present, but there is no significant hyperchromasia or nuclear irregularity or size variation. Mitoses are absent. 1 Patients may have irritation and/or inflammation of the vulva. 2 In one study of 12 cases, HPV was ruled out by polymerase chain reaction and in situ hybridization testing. Herpes was ruled out as well. 1 HPV was also ruled out in another case study. 2 It is thought that the multinucleation represents a fault in nuclear division relating to persistent rubbing of the skin that can occur on either genital or extragenital regions of the body rather than representing the beginning of a neoplastic process. 2 The potential pitfall is overdiagnosing HPV infection based on the multinucleated nature and nucleoli present within these cells.
Conclusions
Mistaking multinucleated atypia for a low-grade, or even a high-grade, squamous intraepithelial lesion can lead to unnecessary therapy. Literature is unavailable on how often this error is made. Multinucleated atypia has not been described as associated with lichen sclerosis or other vulvar dermatoses.
Footnotes
Author Disclosure Statement
There are no conflicts of interest.