
Abstract
Abstract
Objective:
One aim of this article is to present 2 cases of parasitic myomas and 2 cases of leiomyomatosis peritonealis disseminata (LPD) after laparoscopic surgery with electrical morcellation. Other aims include reporting the current authors' incidence and reviewing the literature briefly.
Cases:
In these 4 cases, an electric tissue morcellator was used for myoma removal without any containment technique. All cases were symptomatic and 1 of them also presented with a 3-cm endometrioma nodule in the port site where the morcellator had been introduced in a previous surgery. All of the patients were young (< 40 years). No case of an unsuspected uterine sarcoma was seen.
Results:
The final histopathology was benign in all cases. Currently, all patients are asymptomatic.
Conclusions:
Laparoscopic morcellation of myomas without containment techniques is associated with an increased risk of parasitic myomas or LPD, mainly in reproductive-age women. Techniques for contained morcellation of the uterine tissue should be performed in an attempt to prevent this complication.
Introduction
E
Cases
Four patients initially underwent surgery at the Son Llàtzer Hospital, in Palma de Mallorca, Balearic Islands, Spain, from August 2004 to December 2015. During this period, 92 laparoscopic myomectomies and 239 laparoscopic supracervical hysterectomies (LSH), 123 of them for myomas, were performed. In all cases, an electric tissue morcellator (Gynecare J&J in 1 patient; Karl Storz in the others) was used for tissue removal without any containment technique. The main characteristics of these 4 patients are reported in Table 1.
Patients' Clinical Characteristics with Parasitic Myoma or LPD
Number in parenthesis represents number of myomas.
LPD, leiomyomatosis peritonealis disseminata; LM, laparoscopic myomectomy; IVF, in vitro fertilization; AUB, abnormal uterine bleeding; LSH, laparoscopic supracervical hysterectomy; PG, progesterone; E, estrogen.
The average time between the initial laparoscopic myomectomy and the identification of the parasitic myomas was 47.5 months (range: 20–71 months).
All of these 4 women were symptomatic (Table1). The main symptom that occurred months later was pelvic pain.
Case 1
Only in Case 1 (LPD), the second surgery was performed in another center due to a change in address of the patient. She was the only patient where the approach was laparotomy, and it required the collaboration of a general surgeon because of an injury to a loop of small intestine during resection of one of the parasitic fibroids.
Case 2
In Case 2, a symptomatic endometriotic nodule (3 cm) was resected in a previous port-site (where the mechanic morcellator in the first surgery had been introduced). This patient also presented with an LPD with multiple parasitic myomas in the pelvis, with one of them in the external iliac artery peritoneal surface (Fig 1). There were multiple small myomas in the bladder peritoneum (two of them were subperitoneal) on both paracolic fossas and on the anterior rectosigmal wall. Most of the myomas were resected except some mm-sized myomas on the peritoneal rectal and bladder surfaces.
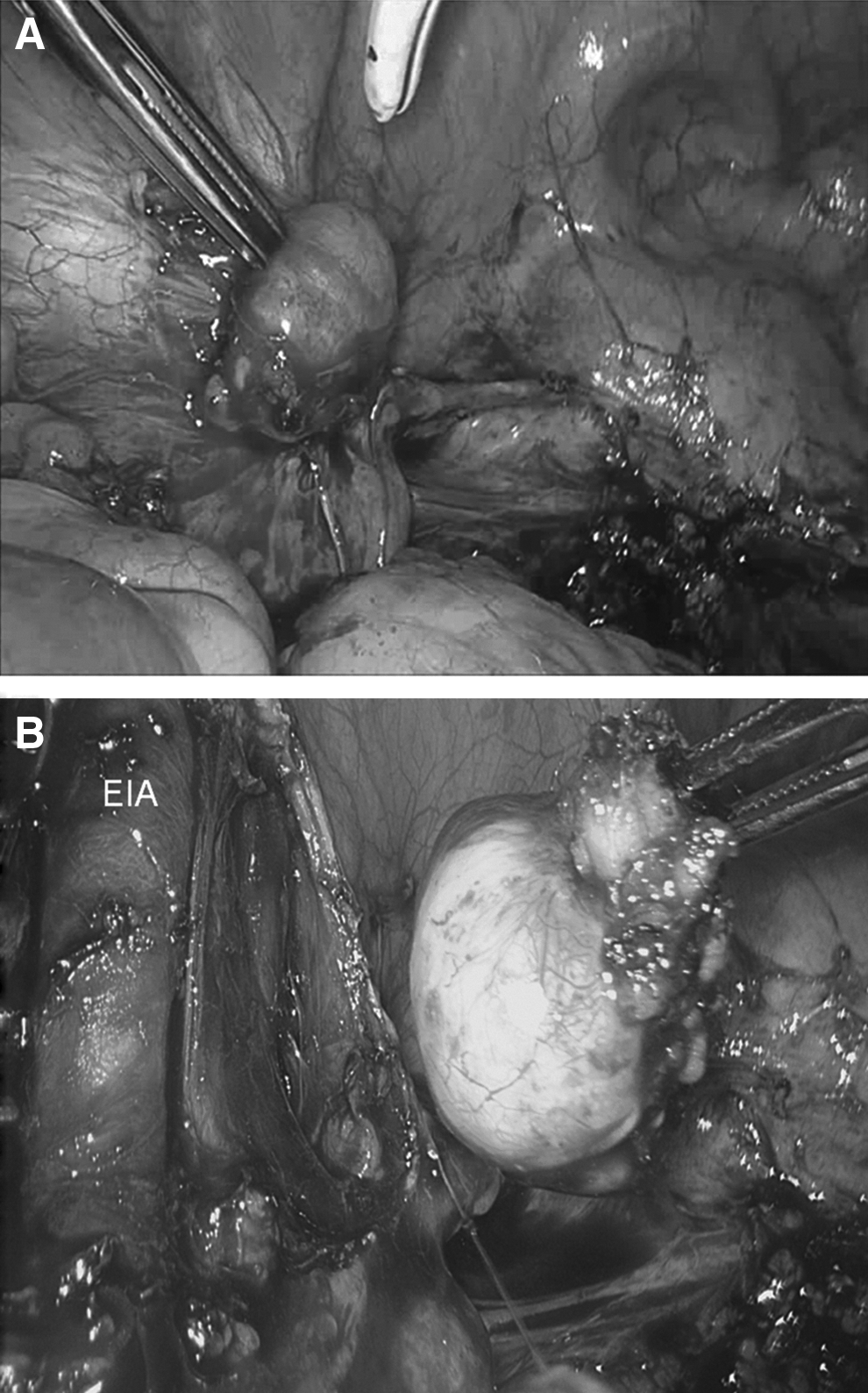
Case 2.
Case 3
Case 3's magnetic resonance imaging (MRI) showed a single parasitic myoma (maximum diameter: 5.4 cm) located on the anterior rectal serous surface (Fig. 2). A laparoscopic myomectomy was performed and, only in this case, the parasitic myoma power morcellation was performed with a completely closed inflated surgical glove. This procedure was carried out with no difficulty. No rectal resection was needed, and after the intervention, this patient's symptoms disappeared.
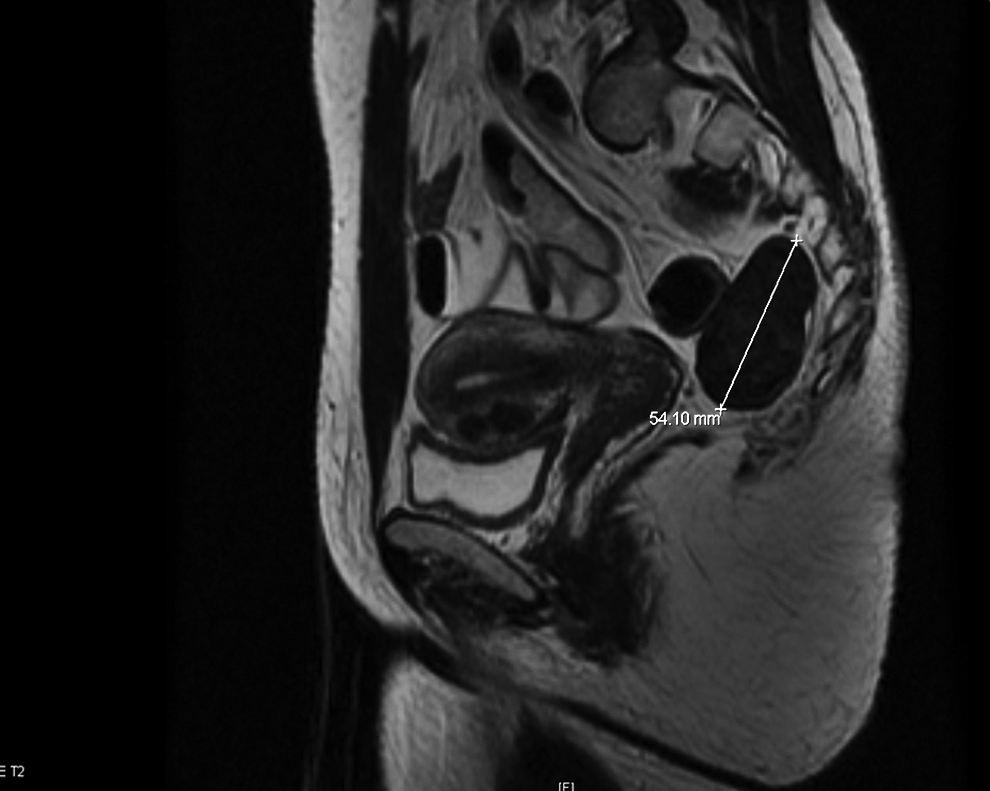
Pelvic nuclear magnetic resonance imaging for Case 3. Parasitic myoma on the anterior sigma wall.
Case 4
Case 4's MRI showed a 4-cm parasitic myoma in the Retzius space (Fig 3). The myoma was extracted by using an endobag and performing a laparoscopic colpotomy (without morcellation).
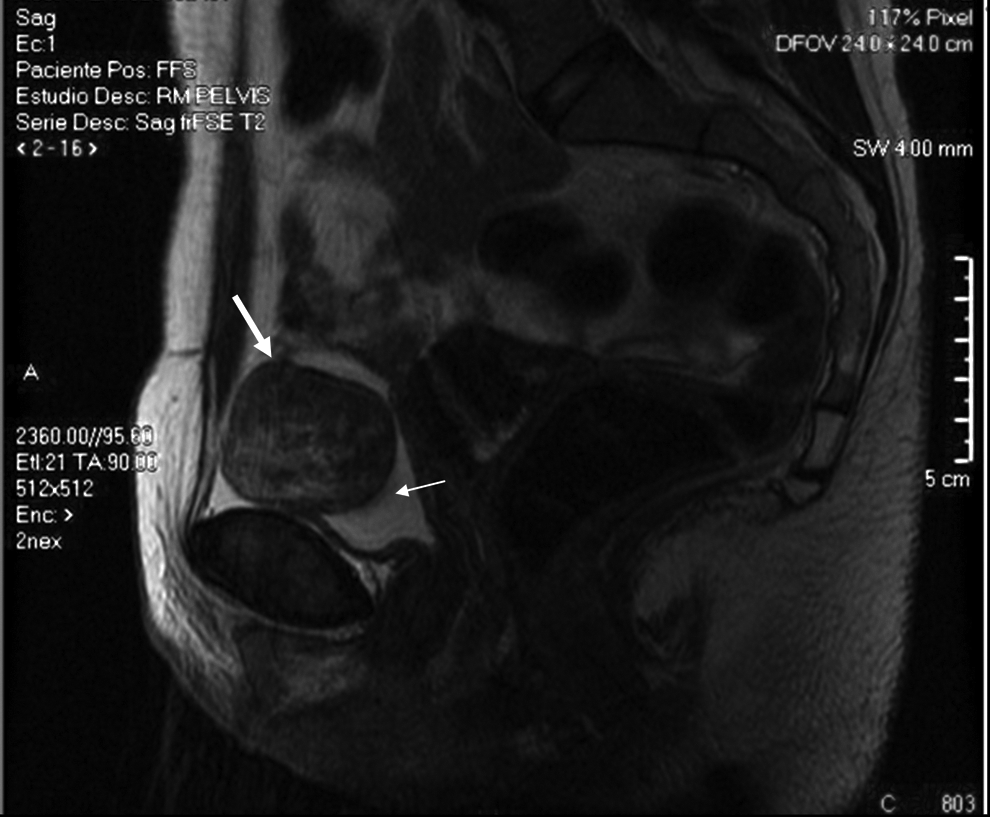
Case 4. Magnetic resonance imaging of a 4-cm parasitic myoma (arrows) in the Retzius space.
Note
In the 2 cases with LPD, almost all the parasitic myomata were resected and a containment bag was used but it was not necessary to perform morcellation because of the small size of the myomas.
Results
The final histopathology was benign in all cases (Table 1). Currently, all patients are asymptomatic.
Discussion
The main reason for not using laparoscopic morcellation in women being treated for uterine fibroids is to reduce the risk of spreading unsuspected cancer. However, there is another complication of laparoscopic morcellation of myomas: the appearance of parasitic myomas and LPD. Parasitic myoma is a condition defined as a myoma with extrauterine nourishing. LPD is a disease that is characterized by the presence of many (sub-)peritoneal smooth-muscle nodules disseminated through the omentum and peritoneum. Although this complication seems to be rare, in the last 15 years, there has been an increase in reports of similar cases in the literature. The first case of a parasitic myoma after using laparoscopic morcellation was reported in 1997. 4 Van der Meulen et al. carried out the most recent systematic review of the literature on the incidence and risk factors of parasitic myomas. 5 In this systematic review, 44 studies were included (31 case reports, 7 case series, and 6 cohort studies) and a total of 69 women with parasitic myoma after laparoscopic morcellation were identified.
The overall incidence of parasitic fibroids after laparoscopic surgery with the use of morcellation is reported to be between 0.12 and 0.95%.5–7 In the current authors' center the incidence of parasitic fibroids after laparoscopic myomectomy was 2.17 %. The incidence of parasitic fibroids after supracervical LSH was 0.83%, and considering exclusively the women who underwent LSH for myomas, the incidence was 1.62%.
The reported incidence of parasitic fibroids after laparoscopic myomectomy was 0.2–1.25%,6,8 but the current authors consider that this incidence may be undervalued because many of these cases may not be published and there probably exist other unknown cases. Thus, according to the literature, 21.7% of cases are often asymptomatic and might be missed, especially in postmenopausal women who no longer have hormonal stimulation. 5 In the current series, the incidence of parasitic fibroids after laparoscopic myomectomy was higher than what had been reported in the literature, but the current authors have been able to determine only the rate of confirmed, symptomatic parasitic myomas.
Until recently, the current authors were not aware of the importance of accurate use of the electric morcellator and of not letting any small tissue fragments become “lost” in the peritoneal cavity. In all cases, electromechanical morcellation was performed inside the abdomen without any containment. In recent years, many centers have used enclosed morcellation and the number of articles describing different techniques has increased.9–11 In Case 3, the current authors used a technique described by Akdemir et al. 12 that consisted of power morcellation performed with a completely closed inflated surgical glove. The current authors think that this is a feasible, inexpensive, and practical technique in which the tissue-extraction procedure can be performed in a completely contained manner. However, there might be a risk of bag perforation or leakage if the glove accidentally breaks and spills its contents into the abdominal cavity. Another limitation of this technique is that it can not be used for larger pieces of 10 cm.
A recent article described a modified method of specimen removal using a tissue pouch and manual morcellation in laparoendoscopic single-site surgery subtotal hysterectomy. 13 Now, with the availability of bags with separate sleeve puncture of the bag that can be ligated before the bag is removed from the abdominal cavity, the procedure seems to be more simple and fairly safe. However, the number of cases and studies are not very high, and some of them are in animal models.14–16
Parasitic myomas are also known as iatrogenic myomas because of the associations among these cases and the histories of laparoscopic surgery using morcellation. The hypothesis that iatrogenic parasitic myomas could develop from retained small tissue fragments after morcellation in the peritoneal cavity is getting stronger. 17 If these fragments are not identified and removed, they could become implanted in any organ or peritoneal surface and form parasitic myomas. Parasitic myomas can also grow in port sites. 3 Case 2 of the current series presented with a 3-cm nodule in the port-site abdominal wall where the current authors thought the nodule was a parasitic myoma but the final histopathology showed that it was endometriosis. The current authors speculate that, during uterine morcellation, a fragment of the endometrium was retained in the abdominal wall when the morcellator cannula was removed.
In addition to single parasitic myomas, some cases of peritoneal leiomyomatosis have been reported, attributing an iatrogenic cause.
18
Three hypotheses have been proposed to explain the pathogenesis of LPD:
Hormonal stimulation promotes the metaplasia of mesenchymal stem cells and could lead to LPD The iatrogenic factor hypothesis suggests that minced fragments of uterine leiomyoma (ULM) created during laparoscopic myomectomy could progress to LPD The genetic theory suggests that ULM could progress to LPD by alteration of the genes related to implantation and proliferation.
Thus, it is possible to distinguish 2 types of LPD: (1) spontaneous and (2) iatrogenic. Iatrogenic disease appears to be related to myomata. A concordant abnormality in the X chromosome and in other chromosomes, including chromosomes 17, 12 and 8, may indicate a common pathogenesis between uterine myomas and LPD. The data suggest that iatrogenic LPD is monoclonal.19,20 Takeda et al. 21 reported peritoneal leiomyomatosis diagnosed 6 years after laparoscopic myomectomy with morcellation with a clearly demonstrable relationship with histopathologic analysis. Yet, spontaneous LPD (in patients without histories of previous uterine surgeries) has been associated with de novo karyotype, 22 progesterone receptor expression, 23 and mutational status discordant with that of the uterine leiomyomas. 24 These findings suggest that spontaneous disease appears to be discordant with myomata.
This type of myoma can be asymptomatic, but, in some cases, this myoma presents with abdominal or pelvic pain, dyspareunia, abdominal distension, urinary frequency, and constipation, and new surgery is necessary. These myomas can be diagnosed long after laparoscopic morcellation, and lesions are commonly multiple and located on the peritoneum of the pelvic or abdominal wall; in the pouch of Douglas; or on the omentum, colon, or small intestines.
Premenopausal status and hormonal-replacement treatment after primary surgery might be considered as risk factors for the development of parasitic fibroids. In a multivariate analysis, age <40 years was found to be a significant risk factor for the development of parasitic myomas. 25 Al-Talib et al. have reported both estrogen and progesterone receptors in LPD cases. 18
In the current series 2 of the 4 patients (in case 1 the second surgery was performed in another hospital and receptors were not studied) presented similar receptor positivity in both samples. In this series all women were under 40 years old, had ovarian preservation, and had endogenous large durations of steroid exposure. For that reason, the current authors would be cautious and avoid myoma morcellation without any containment in women of reproductive age. Laparoscopic management of parasitic myomas is feasible and safe. The histology in all cases described in the literature (also the 4 current cases) has invariably been benign. Although this complication is infrequent, surgeons using minimally invasive techniques should be aware that it exists and should take steps in an attempt to not let it happen.
Conclusions
Although parasitic myomas and LPD after laparoscopic surgery are relatively uncommon, these could be avoidable complications. The real incidence could be higher because of the asymptomatic or unpublished cases. A contained power-tissue morcellation technique should be carried out in all laparoscopic myomectomies, and LSH, especially in younger women who will have an endogenous large duration of steroid exposure as a probable risk factor to develop this complication.
Footnotes
Acknowledgments
The current authors thank and show their gratitude to their colleagues, from the Son Llàtzer Hospital, who provided insight and expertise that assisted the research greatly, although they may not agree with all of the interpretations and conclusions of this article.
The current authors also sincerely thank Dr. Javier Ibarra, MD, for his help in the histologic analysis of the parasitic myomas.
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article.