
Abstract
Abstract
Background:
In young women undergoing radiation therapy for pelvic or low abdominal cancers, ovarian failure is a major concern and every attempt should be made to avoid it. This article describes a case of a young female patient with rectal adenocarcinoma who underwent laparoscopic bilateral ovarian transposition prior to pelvic radiation and chemotherapy.
Case:
A 27-year-old female presented with abdominal pain, diarrhea, and intermittent rectal bleeding of 2 months' duration. Colonoscopy revealed a large frondlike/villous, fungating, ulcerated, nonobstructing mass that was suspicious for malignancy. Biopsy confirmed moderately differentiated rectal adenocarcinoma. The patient elected to undergo laparoscopic ovarian transposition in an attempt to preserve her ovarian function. Subsequently, the patient underwent robotic low anterior resection of the rectum.
Results:
The patient's regular menstruation resumed after surgery, and she has not had any symptoms of ovarian failure or cancer recurrence 2 years after surgery.
Conclusions:
In premenopausal women with pelvic cancers undergoing pelvic radiation, laparoscopic ovarian transposition is a feasible, safe procedure that should be considered to decrease the risk of ovarian failure. (J GYNECOL SURG XXXX:1)
Introduction
T
Case
A 27-year-old nulliparous woman presented to her primary-care physician with abdominal pain, diarrhea, frequent small bowel movements, and intermittent gross hematochezia of 2 months' duration. Her initial workup—which included tests for celiac serologies, stool studies, and erythrocyte sedimentation rate—results were normal. A colonoscopy showed a large frondlike/villous, fungating, ulcerated, nonobstructing mass in the rectum; oozing was present (Fig. 1). Pathology showed a moderately differentiated rectal adenocarcinoma.
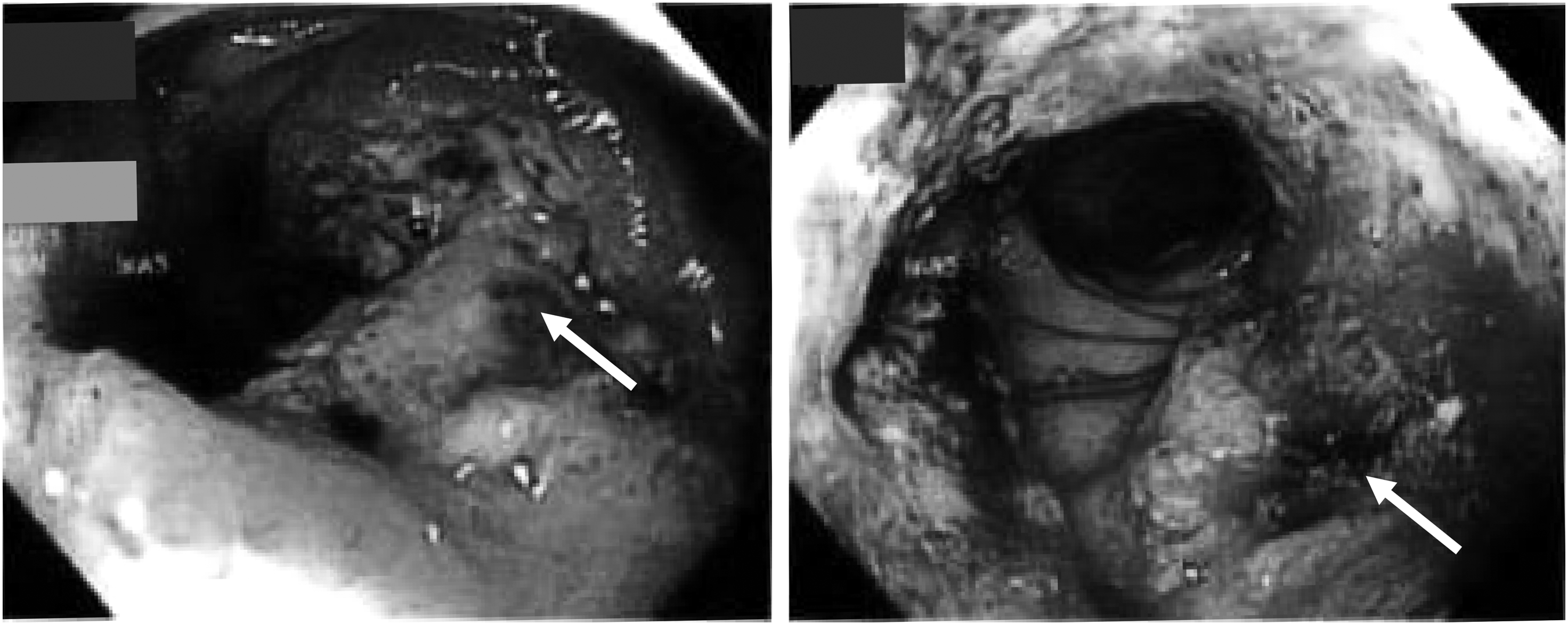
Colonoscopy shows a large frondlike/villous, fungating, ulcerated, nonobstructing mass in the rectum (arrows point to mass).
The patient underwent computed tomography (CT) scans of the chest, abdomen, and pelvis, which showed rectal and inferior sigmoid-wall thickening with ∼6.5 cm of segmental narrowing of the rectum corresponding to the biopsy-proven rectal adenocarcinoma. Multiple perirectal lymph nodes were identified that were worrisome for metastatic involvement. No distant metastasis was noted. Endoanal ultrasound showed an ulcerating circumferential mass in the rectum (1.5 cm in thickness, 3 cm in length) extending to 2 cm from the anal verge. Four malignant-appearing lymph nodes, 8–12 mm in diameter, were visualized endosonographically adjacent to the rectal mass. The clinical diagnosis was staged as cT3, N2, M0 (per the AJCC Cancer Staging Handbook: From the AJCC Cancer Staging Manual, 7th ed.). 4
The institution's tumor board recommended preoperative, neoadjuvant chemoradiation, followed by low anterior resection (LAR) and adjuvant chemotherapy. During consultation with radiation oncology specialists, the patient expressed a strong desire to try to preserve ovarian function and fertility. Ovarian transposition was discussed, along with its potential risks and benefits, and the limited literature regarding the long-term efficacy of the procedure. The patient was made aware that the purpose of ovarian transposition was to decrease the risk of premature ovarian failure and not necessarily to preserve fertility. It was discussed that there was a high likelihood of irreversible uterine/endometrial damage from pelvic radiation that would likely preclude the ability to carry a pregnancy. After thorough discussion of other various options, the patient elected to undergo ovarian transposition.
Laparoscopic lateral ovarian transposition was carried out under general anesthesia. An intraumbilical skin incision was made and a 5-mm trocar was placed under direct visualization. A subxiphoid trocar was inserted under laparoscopic guidance to the left of the falciform ligament. Two 3-mm trocars were inserted in the right and left lumbar regions at the level of the umbilicus to provide good access for high lateral ovarian transposition. The patient was placed in the Trendelenburg position and the small bowel was retracted into the upper abdomen. The abdominal–pelvic cavity was examined. The rectosigmoid was markedly distended due to partial obstruction with the rectal mass. Peritoneal washings were obtained for cytology. The level of the aortic bifurcation at L4–L5 was noted and was traced laterally to the lateral abdominal wall and the paracolic gutters. Markings were made in the peritoneum using monopolar energy, marking the lowermost point of the targeted new position for the ovaries.
The procedure was initiated by taking down the rectosigmoid attachments at the white line of Toldt. The pelvic brim was adequately exposed and the left infundibulopelvic (IP) ligament and left ureter were noted. The patient had expressed interest in preserving the fallopian tubes. The left fallopian tube was separated from the left ovary using a vessel-sealing cutting device with careful attention to avoid injury to the fallopian tube, the ureter, and the IP vessels. The utero-ovarian ligament was coagulated and transected with care to maintain an adequate blood supply to the fallopian tube. Noting the IP insertion into the hilum of the ovary, care was taken to avoid injury to the ovarian blood supply. The peritoneum lateral to the left IP was opened and the incision was extended cephalad toward the left lateral peritoneal marking in the paracolic gutter. The left IP ligament was skeletonized and separated from the ureter with a combination of blunt dissection and electrosurgery as needed. The sigmoid was deflected medially and the plane between the left ureter and the left IP was dissected all the way up to the paracolic gutter. The IP ligament and the ovary were deflected cephalad and the undersurface of the IP was dissected off the iliac vessels and the psoas muscle.
The dissection was continued cephalad until the ovary was able to reach the marking at the level of L4. A small peritoneal incision was then made in the paracolic gutter. A retroperitoneal tunnel was created and the ovary was grasped and pulled through the tunnel. Care was taken to avoid kinking or twisting the ovarian vessels. The ovary was brought out through the peritoneal window and was sutured to the peritoneum and transversalis fascia using 2-0 silk on a CT1 needle at 3 points, avoiding the IP vessels and the hilum of the ovary (Fig. 2). Two hemoclips were placed at the lower-most point of the ovary for later identification during radiation simulation (Figs. 3 and 4). Excellent suspension and hemostasis were noted. The right ovary was subsequently transposed in a similar fashion after deflecting the cecum medially.
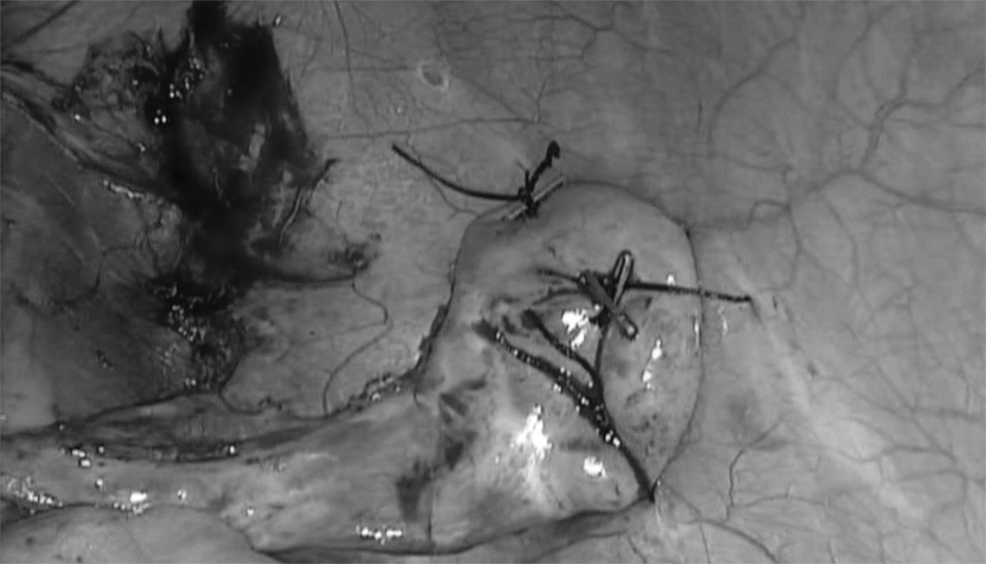
The transpositioned ovary is sutured to the transversalis fascia at three points, using permanent sutures. Hemoclips are applied for identification during radiation.

The transposed ovaries at their final location (shown by the arrows) of L3-L4 upon radiation simulation.

Radiation simulation showing the transposed ovaries (arrows) and their location in relationship to the planned radiation field.
With this procedure, preservation of the anatomical location of the fallopian tube was accomplished. Although the exact rate of spontaneous pregnancy and the risk of ectopic pregnancy remain unknown, multiple studies have reported spontaneous pregnancy following lateral ovarian transposition when accompanied with tubal preservation.5,6 The current patient requested tubal preservation, with the understanding of the above caveats. The utero-ovarian vessels are preserved as much as possible to provide adequate blood supply to the tubes. To do this, the vessels are sealed and cut flush with the ovary on the utero-ovarian side. In addition, a plane is developed between the mesosalpingeal vessels and the ovarian vessels at the ovarian hilum.
This patient subsequently underwent treatment planning for radiation therapy. The ovaries were contoured on the CT scan. Dose–volume histogram analysis showed a mean dose of 4.7 Gray (Gy) to the left ovary and 7.2 Gy to the right ovary. The patient was treated with a dose of 45 Gy in 25 fractions to the pelvis, using an intensity-modulated radiation therapy technique. Prior to receiving pelvic radiotherapy, the primary tumor was given a boost of 5.4 Gy in three fractions, using a three-dimensional conformal technique due to the need to deliver emergent treatment for acute symptoms of rectal obstruction. The patient also received concurrent chemotherapy with capecitabine during her course of radiation therapy. Figures 3 and 4 show the positions of the ovaries in the abdomen and in relation to the radiation fields.
Results
Four weeks after the completion of neoadjuvant chemoradiotherapy, this patient underwent robotic LAR with a diverting ileostomy. The patient then received 4 months of adjuvant chemotherapy (Xeloda® and oxaliplatin) and underwent reversal of the ileostomy 2 months after her last course. The patient's regular menstrual cycles resumed before initiating adjuvant chemotherapy. Two years after treatment, this patient continues to have regular cycles and never experienced any menopausal symptoms.
Discussion
With modern advances in early detection and multidisciplinary approaches to treatment, mortality rates of cancer have decreased in the United States. 7 In contrast to the decline in overall mortality related to cancer, the incidence of certain cancers, including colorectal cancers, has increased in adults younger than 50 years of age. 8 Primary colorectal cancer has been associated with metastases to the ovaries, although the frequency is low. 9 Radiation and chemotherapy can both reduce ovarian function, leading to premature ovarian failure, causing osteopenia and osteoporosis, significant menopausal symptoms, and compromised fertility. An analysis of 162 premenopausal women with colorectal cancer who underwent adjuvant chemotherapy and chemoradiotherapy revealed that >90% of patients with rectal cancer experienced long-term amenorrhea. 10 Radiation can hasten the natural atresia of ovarian primordial follicles. Chemotherapy can also be detrimental to the ovaries. Certain chemotherapeutic agents can increase the loss of ovarian primordial follicles and accelerate the process of reproductive aging.
Multiple studies have reported preservation of ovarian function following ovarian transposition, chemotherapy, and radiation. Huang et al. reported on 6 of 7 patients, younger than 40 years of age, with pelvic malignancies who retained ovarian function as evidenced by follicle-stimulating hormone levels. 11 In a meta-analysis, Gubbala et al. reported that ovarian transposition was associated with ovarian function preservation in 90% of patients, based on a number of clinical and laboratory data. 12 In a prospective study of 107 patients with cervical cancer, patients underwent bilateral ovarian transposition before surgery, vaginal brachytherapy, and/or external radiation therapy. The researchers concluded that the rates of ovarian function preservation differed depending on the type of radiotherapy; 90% of patients who underwent vaginal brachytherapy and 60% of patients who underwent external radiation therapy with vaginal brachytherapy had preserved ovarian function. 13
Reproductive success following ovarian transposition has also been reported. One study reported 14 spontaneous pregnancies in 11 women treated for Hodgkin's lymphoma over the course of 14 years. 14 Surrogate pregnancies, using oocytes retrieved transabdominally from patients following ovarian transposition and cancer treatment, have also been reported in the literature.15–18
Many patients with cancer do not receive adequate information regarding their options for ovarian function preservation. Lack of physician knowledge regarding options and resources for ovarian function preservation and concerns about cost and delaying the initiation of cancer treatment are barriers to appropriate care of these patients. 19 Women with cancer are interested in discussing options for ovarian function and fertility preservation. 20 Collaborative care between an oncology team, a psychologist, a fertility specialist, and a skilled gynecologic surgeon, as well as involving the patient and her family can be very beneficial to any woman who wishes to have access to these options.
Conclusions
Laparoscopic ovarian transposition is a safe procedure that should be recommended to patients undergoing treatment for pelvic cancers to reduce the risk of ovarian failure and infertility. The rare use of the procedure mandates the need for well-designed clinical trials in an effort to optimize cancer treatment, so that preservation of ovarian function is a priority throughout the course of cancer care and remission.
Footnotes
Author Disclosure Statement
All authors of this article report no financial disclosures or conflicts of interest related to this study.