
Abstract
Abstract
Background:
The field of minimally invasive surgery is progressing rapidly and extends to the field of gynecologic oncology. To date, the number of gynecologic oncologists who use laparoscopic surgery to treat endometrial cancer is increasing. As minimally invasive therapy advances technically and instrumentally, more-complicated procedures are being performed, thereby increasing the number of complications. Vaginal cuff dehiscence (VCD) is one of complications that may arise. VCD is a rare but severe complication.
Case:
A nonobese 55-year-old female underwent laparoscopic hysterectomy, bilateral salpingo-oophorectomy, and dissection of pelvic and para-aortic lymph nodes for endometrial cancer. Subsequently, this patient underwent total laparoscopic repair of VCD during chemoradiation that was used to treat her endometrial cancer following the laparoscopic staging.
Results:
After the second surgery, this patient received 2 cycles of chemotherapy without brachytherapy, and follow-up examination did not show any evidence of recurrence.
Conclusions:
Radiation therapy may impair wound healing and affect surgical outcomes; thus, the treatment of VCD should be decided by the patient's general condition, including any evisceration, and assessment of her risk factors. (J GYNECOL SURG 33:77)
Introduction
A
Case
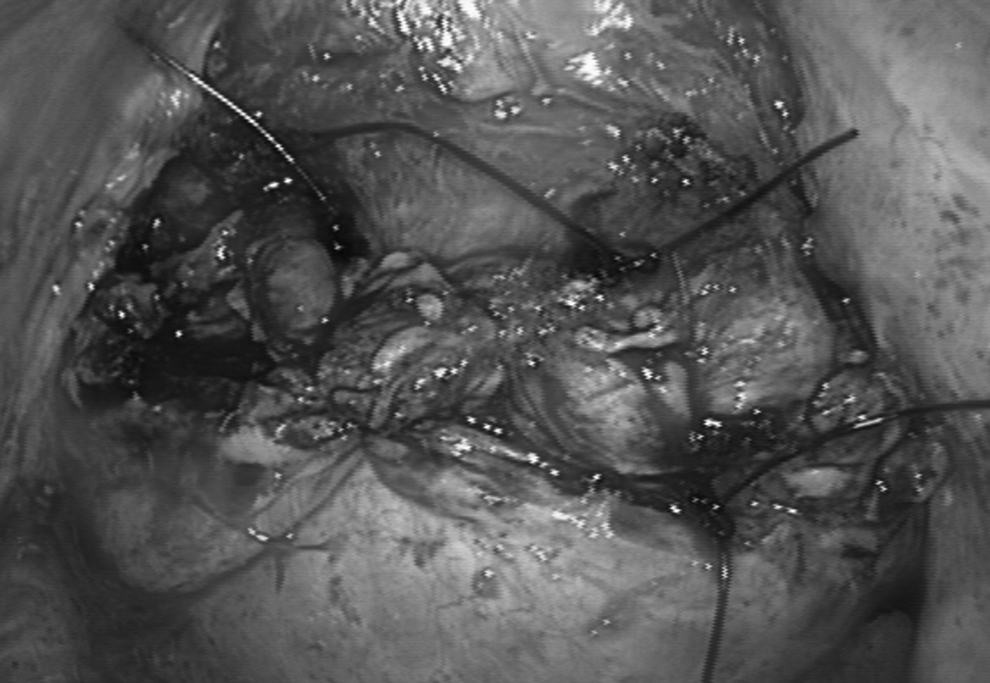
A nonobese 55-year-old female underwent laparoscopic hysterectomy, bilateral salpingo-oophorectomy, and dissection of pelvic and para-aortic lymph nodes for endometrial cancer. The vaginal cuff was incised using monopolar electrocautery and was closed with 1-layer full-thickness vaginal cuff closure, using an 0-Vicryl suture in a running fashion. Prophylactic antibiotics were administered before and during surgery. Final pathology testing revealed endometrioid adenocarcinoma, grade 2, pT1bN1M0, International Federation of Gynecology and Obstetrics stage C2. It was recommended that this patient receive extended field radiation therapy and brachytherapy 8 weeks postsurgery and chemotherapy (cisplatin, 60 mg/m2; epirubicin, 60 mg/m2; every 3 weeks for 6 cycles) to be started 2 weeks postoperation. During extended field radiotherapy therapy and after 4 cycles of chemotherapy, the patient noticed an extrusion from her vagina. An examination revealed VCD with small bowel at the vaginal opening (Fig. 1). There were no signs of incarceration or any symptoms of infection.

Vaginal cuff dehiscence (VCD) with small bowel. Examination revealed VCD with small bowel at the vaginal opening.
On that day, the patient underwent urgent laparoscopic surgery. There was a 3-cm horizontal defect on the vaginal vault, and the edge of her vagina was thin (Fig. 2). The bladder was separated from the vaginal cuff, and the fibrotic tissue was sharply dissected and excised circumferentially. Two-layer repair, with interrupted stitches, using a Prolene® 0 suture, was performed; it did not include the uterosacral or cardinal ligaments (Fig. 3).

Defect on the vaginal vault. There was a 3-cm horizontal defect on the vaginal vault, and the edge of vagina was thin.
Repair of vaginal vault. Two-layer repair with interrupted stitches using Prolene® 0 suture was performed.
Results
After the second surgery, this patient received 2 cycles of chemotherapy without brachytherapy, and follow-up examination did not show any evidence of recurrence.
Discussion
Minimally invasive surgery contributes to the quality of life of patients who undergo hysterectomy; however, some potentials for complications increase after robotic or laparoscopic hysterectomies. VCD is a rare but severe complication of these surgeries. The rates of VCD are 0.64%–4.1% robotically, 0.47%–4.93% laparoscopically, 0.13%–0.29% vaginally, and 0.12%–0.99% abdominally.1–3 Many researchers have proposed that the difference of VCD rates results from the use of thermal energy devices for colpotomy and from the way the vagina is closed.1,3
On the contrary, Uccella et al. reported that VCD was not caused by the use of electrosurgery, according to a multi-institutional analysis of >12,000 hysterectomies; rather, VCD was the result of the vaginal closure technique used. 4 Kim et al. also reported that VCD rates were 5.79% for total laparoscopic hysterectomy and 1.68% for laparoscopic-assisted vaginal hysterectomy, and that this difference was caused by the method of suturing the vaginal cuff. 5 Furthermore, Kim et al. divided total laparoscopic hysterectomies into two groups according to the manner of vaginal cuff closures. The researchers reported that intracorporeal cuff suture was superior to vaginal suture for preventing VCD (intracorporeal continuous suture VCD was 2.96%, and vaginal continuous suture VCD was10.47%).
Kashani et al. reported that VCD rate can be decreased by closing the vaginal cuff vertically and incorporating at least 10 mm of pink tissue, full-thickness vaginal edges. 6 In the current case, the edge of vagina was thin, and VCD was caused by the manner of vaginal closure and by chemoradiation therapy. To reinforce vaginal closure, delayed absorbable monofilament sutures were used and a 2-layer cuff closure was made. Similar to this case, for which radiation therapy was needed after surgery, vaginal suture techniques incorporating full-thickness and adequate depth of the vaginal edge and 2-layer cuff closure are required. These vaginal suture techniques could minimize the risk of VCD 7 ; however, a large prospective study has to be carried out with a sufficient number of cases.
Ten cases of VCD following laparoscopic or robotic hysterectomy and radiation therapy were found in the literature.8–11 Three cases were post–robotic hysterectomy for endometrial cancer and occurred 6–9 weeks after surgery and also occurred during the radiation treatment simulation when using a vaginal cylinder. During vaginal brachytherapy, significant pressure from cylinder insertion may cause dehiscence. Six cases were robotic surgeries and 1 case was a laparoscopic radical hysterectomy. Of the 10 patients, 7 patients required surgical closures; the other 3 were allowed to heal via secondary intention.
The current authors had a case of spontaneous healing of VCD in a patient with uterine cervical cancer following laparoscopic radical hysterectomy and chemoradiation. The nonsurgical method was chosen because the current authors considered that the repair of that patient's vagina might affect the wound healing because of her postradiation therapy and radical hysterectomy. However, in the current case, VCD occurred during adjuvant therapy and it was necessary to restart the patient's chemotherapy as soon as possible.
Conclusions
Treatment of VCD—surgical or nonsurgical, whether the route is through the vagina or transabdominal—can be decided according to the patient's general condition, including any evisceration, and assessment of her risk factors.
In patients who undergo laparoscopic hysterectomy and possible radiotherapy, the current authors recommend 2-layer, full-thickness vaginal cuff closure, including at least 10 mm of tissue from the vaginal edge, using a delayed monofilament suture to prevent VCD.
Footnotes
Acknowledgments
The authors thank the Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital for Dr. Kusunoki.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.