
Abstract
Abstract
Objective:
Laparoscopy is increasingly the preferred surgical approach in patients with ectopic pregnancy. The aim of this research was to evaluate the feasibility, safety, and outcomes of surgery for tubal ectopic pregnancy using single incision laparoscopic surgery (SILS) in comparison to conventional laparoscopic surgery (CLS) in the authors' local setting.
Design:
This single-center prospective study included consecutive patients treated by the SILS or CLS approach for salpingectomy in tubal ectopic pregnancy from September 1, 2011, to April 1, 2016.
Materials and Methods:
Information on patient bio-data, intra-, and postoperative data were collected and compared between patients who underwent the two surgical approaches.
Results:
In total, 93 consecutive patients underwent surgery for salpingectomy in tubal ectopic pregnancy. Of these, 33 (Group 1) were treated by SILS and 60 (Group 2) were treated by standard CLS. All 33 (100%) patients were treated successfully with the SILS approach, without need for conversion to CLS or laparotomy. No significant differences were found in mean operative time (56.1 ± 22.2 minutes versus 55.0 ± 17.4 minutes), length of hospital stay (1.45 ± 0.794 days versus 1.83 ± 1.12 days), and patient satisfaction score (8.5 ± 0.837 versus 7.9 ± 0.1) between the SILS versus the control group. No complications were encountered in either group.
Conclusions:
SILS appears to be a safe and feasible alternative to CLS for treatment of tubal ectopic pregnancy in suitable patients. Outcomes on operative times, hospital stays, satisfaction scores, and complication rates were at least equivalent to CLS. Future researchers may wish to compare patient satisfaction among patients who underwent SILS versus CLS more holistically. (J GYNECOL SURG 33:61)
Introduction
E
Continued efforts to reduce the number and size of ports, lessen perioperative morbidities, and improve cosmetic outcomes led to the emergence of single incision laparoscopic surgery (SILS).7–37 SILS is reported to be feasible and safe in certain gynecologic conditions7–24 as well as in urology26–32 and colorectal surgery.33–37 To date, three studies7–9 have investigated outcomes of the use of SILS in tubal ectopic pregnancy in comparison to conventional laparoscopy, while other researchers10–16 have discussed SILS use in other forms of ectopic pregnancy or in conjunction with specific surgical techniques. SILS seems to be particularly suited for the surgical treatment of ectopic pregnancy as the majority of patients are young and relatively healthy, and are likely to be interested in improved cosmesis and reduced morbidity postsurgery. In addition, SILS can be easily recoursed to conventional laparoscopy if necessary, without compromising the safety of patients.
The current authors hope to shed light on the outcomes of SILS in comparison to CLS for tubal ectopic pregnancy in Singapore. The current authors also took a cue from Yoon et al. 7 to explore the subjective outcome of SILS further in comparison to CLS, which the current authors assessed through a patient-reported satisfaction score, obtained from each patient at least 3 days after the surgery.
The current authors postulate that an assessment on the feasibility of SILS in comparison to CLS for tubal ectopic pregnancy would potentially be useful and practice-changing in the surgical management of tubal ectopic pregnancy in their local setting.
Materials and Methods
Study design
This single-center prospective observational study was performed to examine the feasibility and safety of SILS in the surgical treatment of tubal ectopic pregnancy in Singapore. From September 1, 2011, to April 1, 2016, women diagnosed with tubal ectopic pregnancy at the National University Hospital were offered the option of surgical treatment by the SILS or CLS approach, performed by a single surgeon. The ultimate surgical approach used was determined by each patient. Ethical approval was obtained from the National Health Group Domain-Specific Review Board of the hospital.
For inclusion in the study, women had to be hemodynamically stable and diagnosed with tubal pregnancy, defined as: (A) transvaginal ultrasound visualization of a gestational sac containing a yolk sac and/or fetal pole in the adnexa; (B) no intrauterine gestational sac with an adnexal mass and a human chorionic gonadotropin (hCG) level >2000 mIU/mL; or (C) no intrauterine gestational sac with an adnexal mass and a plateaued serum β-hCG pattern.
A single surgeon who is skilled in the CLS approach with experience in excess of 1000 CLS procedures, performed the salpingectomy, using either the SILS or CLS approach for tubal ectopic pregnancy.
SILS for tubal ectopic pregnancy
In SILS for the surgical treatment of tubal ectopic pregnancy, each patient was placed in a lithotomy position and surgery was performed under general anesthesia. A 1–1.5-cm longitudinal incision was made at the umbilicus. The peritoneal cavity was entered, using the open Hasson entry method. A multichannel SILS port was then inserted at the umbilicus to achieve pneumoperitoneum at 15 mm Hg. Several different systems (Fig. 1) have been developed to facilitate pneumoperitoneum in SILS, such as the Covidien SILS® Port (Fig. 1A), Olympus Triport® (Fig. 1B), and Karl Storz X-Cone® Device (Figure 1C), on top of single bent laparoscopic graspers (Fig. 1D).
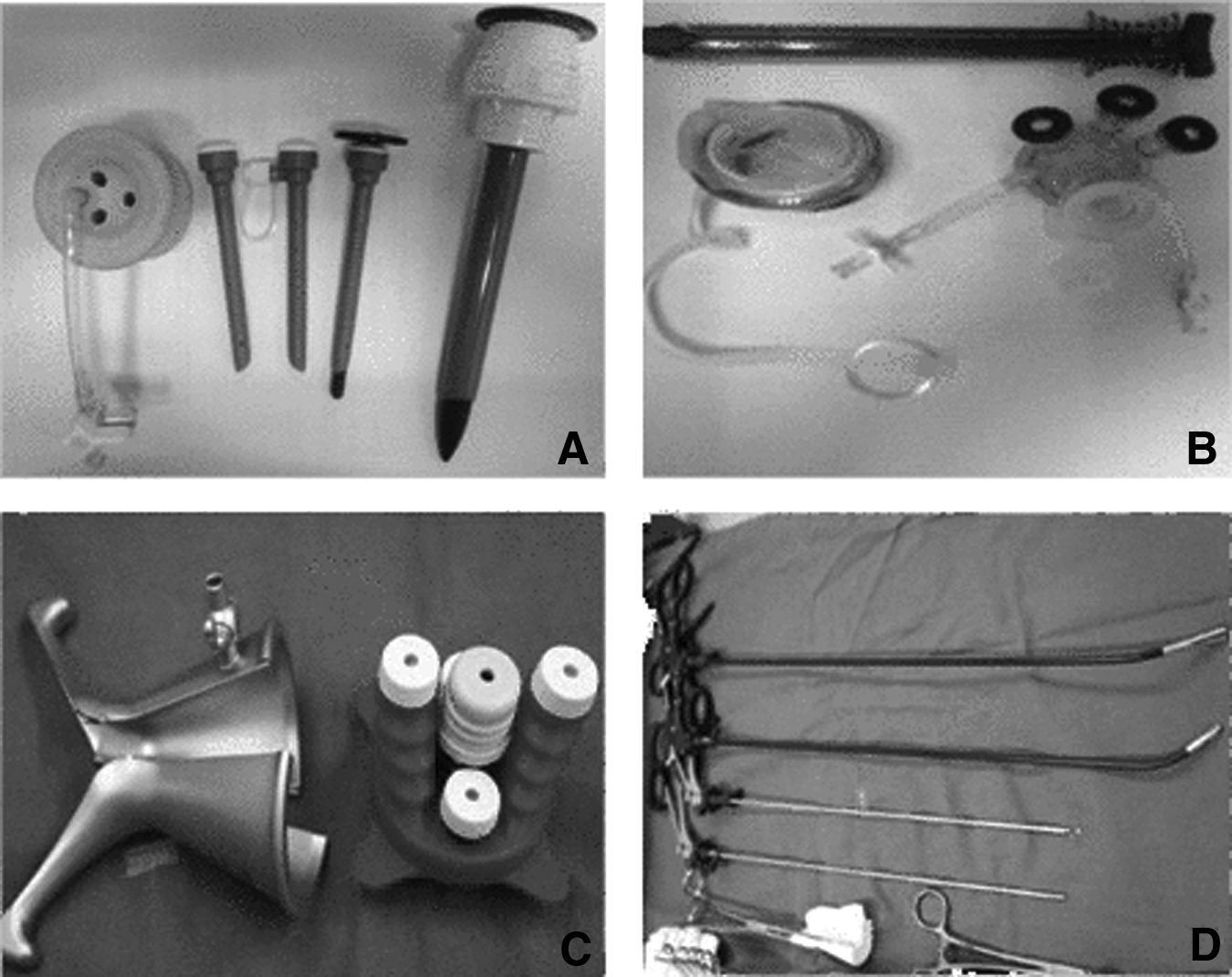
Single ports from various companies used in the study and laparoscopic graspers.
Initial peritoneal surveillance with evacuation of the clots was performed to expose the pelvis and identify the ectopic pregnancy (Fig. 2A). The ectopic pregnancy was grasped (with Clickline® single bent grasping forceps from Karl Storz), and bipolar diathermy was applied to the proximal and distal ends of the affected tube (Fig. 2B). Once the bleeding was controlled, the mesosalpinx was excised in a fashion parallel to the fallopian tube (Fig. 2C). The specimen was then placed into the Endo Catch

Salpingectomy for tubal ectopic pregnancy using single incision laparoscopic surgery approach.
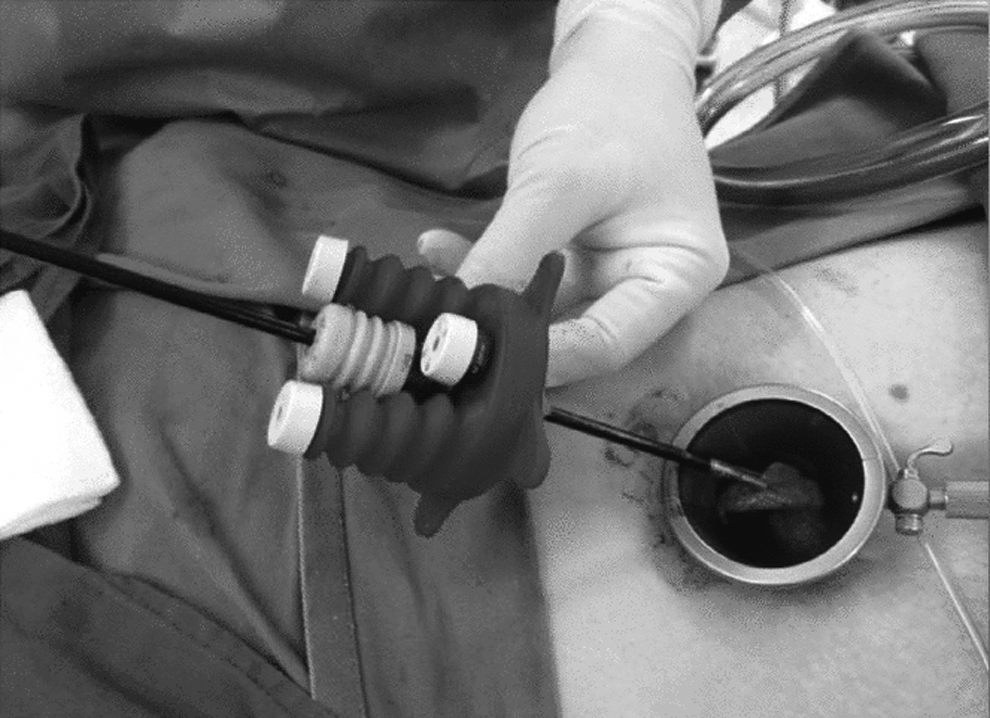
Retrieval of specimen via umbilical incision.
After the surgery, the single incision at the umbilicus was small (Fig. 4A) and resulted in a well-hidden scar that is almost unnoticeable after recovery in 4 weeks (Fig. 4B).
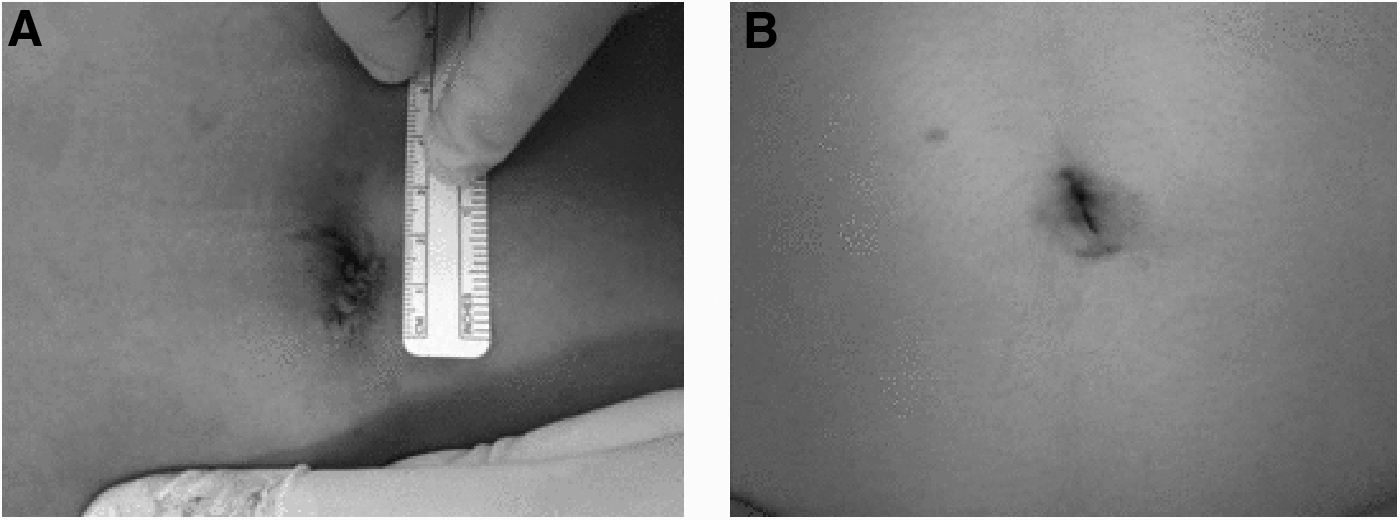
Surgical incision postsurgery.
Study procedure
Patient demographics, preoperative evaluation, intra- and postoperative data of patients who underwent surgical treatment for ectopic pregnancy from September 1, 2011 to April 1, 2016, were extracted from hospital electronic patient records and patient case files. The data of patients treated by SILS (Group 1) were compared to a control group of patients treated by CLS (Group 2).
An assessment of subjective postoperative outcome was also included in the form of a patient satisfaction score, scaled from 0 (“least satisfied”) to 10 (“most satisfied”). To obtain this score, patients were asked: “From a scale of 0 to 10, where 0 is least satisfied and 10 is most satisfied, what is your level of satisfaction with this surgery?” This was obtained through telephone calls to the patients, to inquire about their levels of satisfaction with their surgeries after they had been discharged from the hospital, at least 3 days postsurgery.
Statistical analyses were performed using the Statistical Package for the Social Sciences Version 12.0 (SPSS Inc., Chicago, IL). An independent t-test was used to compare continuous parametric variables, and a χ2 test was used for categorical variables. A p-value of ≤0.05 was considered to be statistically significant.
Results
In total, 93 patients were included in the study, with 33 cases of SILS (Group 1) and 60 cases of CLS (Group 2). No significant differences were found in age, body mass index (BMI), parity, ethnicity, and nationality of both groups (Table 1).
SILS, single incision laparoscopic surgery; CLS, conventional laparoscopic surgery; BMI, body mass index.
However, a significant difference was found in the site of surgery. In Group 1, salpingectomies were performed mostly on the left (51.5%), followed by the right (39.4%) and bilaterally (9.1%), while, in Group 2, most were on the right (61.7%) and the rest were on the left (38.3%; p = 0.016). However, albeit statistically significant, the site of surgery has no clinical significance and should not be expected to affect postoperative outcome significantly. Surgical instruments used for Group 1 and 2 also differed. In Group 1, SILS was done with Covidien SILS Port (21.2%), Olympus Triport (21.2%), and Karl Storz X-Cone Device (57.6%). CLS in Group 2 was performed with standard conventional laparoscopic instruments (100.0%). See Table 1.
No significant differences were observed between the two groups with respect to preoperative blood hemoglobin (g/dL), preoperative serum β-hCG (mIU/mL), mean length of ectopic mass by ultrasound (cm), presence of previous abdominal surgery, and need for preoperative blood transfusion. See Table 2.
SILS, single incision laparoscopic surgery; SD, standard deviation; CLS, conventional laparoscopic surgery; hCG, human chorionic gonadotropin.
No significant differences were observed between the two groups on intraoperative findings of ruptured ectopic pregnancy or presence of adhesions (Table 3). The levels of hemoperitoneum (mL) and operative time (minutes) of both groups were comparable. Group 1 had a slightly longer operative time (minutes) of 56.1 ± 22.2 versus 55.0 ± 17.4 (p = 0.784). See Table 3.
SILS, single incision laparoscopic surgery; SD, standard deviation; CLS, conventional laparoscopic surgery.
In terms of postoperative outcomes, length of hospital stay (days), and patient satisfaction score, both groups had no significant differences. Group 1 had a marginally shorter length of hospital stay of 1.45 ± 0.794, compared to 1.83 ± 1.12 for Group 2. Satisfaction score of Group 1 was 8.5 ± 0.837, which was slightly higher than that of 7.9 ± 0.775 for Group 2, which may be explained by better cosmetic outcome postsurgery. See Table 4. In both groups, blood loss was minimal, and no complications, such as bowel injury or wound infections, occurred after surgery.
SILS, single incision laparoscopic surgery; SD, standard deviation; CLS, conventional laparoscopic surgery.
Discussion
SILS is a new innovative laparoscopic technique that has rapidly gained recognition for various indications in the field of gynecology. Undeniably, SILS offers a superior cosmetic outcome, as the single umbilical incision can be well-hidden after recovery. An increasing number of recent studies have concluded SILS feasibility and safety in various disciplines, thus leading to its increased application.7–37
SILS appears to be suited for gynecological procedures of intermediate complexity, such as salpingectomy for tubal ectopic pregnancy, for which there is minimal dissection and no requirement for suturing. We believe that the lack of surgical experience in our first attempt with SILS, in addition to the emergency setting of the surgery, was likely the cause of the marginally longer operative time in the SILS group, compared to the conventional group, although the difference was not statistically significant. With more experience, the duration of surgery in the SILS group is likely to be gradually reduced.
The major technical difficulties of SILS were reduced triangulation, which led to limited space for lateral traction, and in-line viewing and external clashing of instruments, as all the instruments were located in parallel. This unfavorable ergonomic position often resulted in prolonged surgical duration.
However, the use of a single bent laparoscopic grasper (a Clickline single bent grasping forceps from Karl Storz) improved the triangulation and traction required in SILS, thus facilitating the surgery. The long length 30° telescope reduced external clashing of the hands and instruments. Light intensity was reduced due to the longer length of the telescope. Since the procurement of these surgical instruments, there was a decrease in the duration of the operation. In addition, no problems were encountered during the evacuation of the hemoperitoneum and visualization of the contralateral adnexa in the current authors' experience, which supports findings by Marcelli et al. 8
Yoon et al. 7 conducted a similar study with 3 skilled surgeons performing surgeries using the SILS approach, using their own self-assembled system. No failures or complications were reported. Results of the current study were similar. However, the SILS procedures in this study were performed by the same surgeon but with different port systems. The current authors did not find any technical advantages among the various port systems, except that the Karl Storz X-Cone Device has added benefits of low cost and reusability. Uterine manipulation improved exposure of the adnexa, and the current authors concur with Marcelli et al. 8 that a simple uterine manipulator (e.g., a Hegar dilator or curette) was sufficient.
Study limitations
The current study had a relatively small sample size for the SILS group with a larger control group. In addition, no objective assessment of the cosmetic outcome of the patients' scars was performed in this study, although this is supposedly the biggest advantage of SILS. The current authors were also limited by their inclusion criteria that restricted cases to tubal ectopic pregnancy and the surgical method of salpingectomy. As patients requiring other types of surgery for ectopic pregnancy are relatively rare, future studies with multiple centers are needed for a better comparison.
Conclusions
The current study demonstrated that outcomes for operative times, hospital stays, satisfaction scores, and complication rates of SILS for salpingectomy in tubal ectopic pregnancy were at least equivalent to CLS. The advent of SILS calls for a need to improve standards and to consider offering SILS to suitable patients presenting with tubal ectopic pregnancy. This offer can be done even in cases of significant hemoperitoneum, as shown in this study. With the increasing number of positive reports on the feasibility and safety of SILS, the current authors believe that it is timely to offer SILS as a recommended surgical option in the treatment of tubal ectopic pregnancy. Future researchers may wish to compare patient satisfaction among those who underwent SILS versus CLS more holistically, by including separate scores for domains such as patient-reported levels of postoperative pain; number of days required before return to usual activities; and satisfaction with scars at 1 week, 4 weeks, 3 months, and 6 months after surgery.
Footnotes
Author Disclosure Statement
All authors have no conflicts of interest to report.