
Abstract
Abstract
Background:
Squamous-cell carcinoma (SCC) of the ovary arising from an epidermoid cyst is an exceptionally rare occurrence. SCC presenting with a metastatic nodule in the myometrium has not yet been reported in literature. Most commonly, SCC arises from mature cystic teratomas of the ovaries. It presents with nonspecific signs and symptoms in postmenopausal females.
Case:
This article reports on a case of pure SCC of the ovary with metastasis to the myometrium in a 55-year-old postmenopausal female that was diagnosed on a histopathologic examination.
Results:
Histopathologic examination led to the diagnosis of well-differentiated SCC originating from the epidermoid cyst of the ovary and metastasizing to the uterus.
Conclusions:
Preoperative radiologic diagnosis is challenging; hence, postoperative histopathologic examination is essential for a final diagnosis. Serum markers, such as SCC antigen and CA-125, help in making a provisional diagnosis of SCC. Due to the rarity of such cases in the literature, treatment options are not clearly understood. (J GYNECOL SURG 33:156)
Introduction
S
Case
A 55-year-old female presented with abdominopelvic pain and a mass she had for 1 month to a gynecology outpatient department. There was no significant past medical history and menstrual history. Physical examination revealed a soft abdomen with tenderness and a palpable mass in the right lower quadrant. Pelvic examination revealed 2-week–sized uterus and a palpable right adnexal mass. Her tumor markers—such as β–human chorionic gonadotropin, α-fetoprotein, and lactate dehydrogenase—were within normal limits. The patient underwent a planned exploratory laparotomy with a total abdominal hysterectomy, with a bilateral salpingo-ophorectomy and omentectomy.
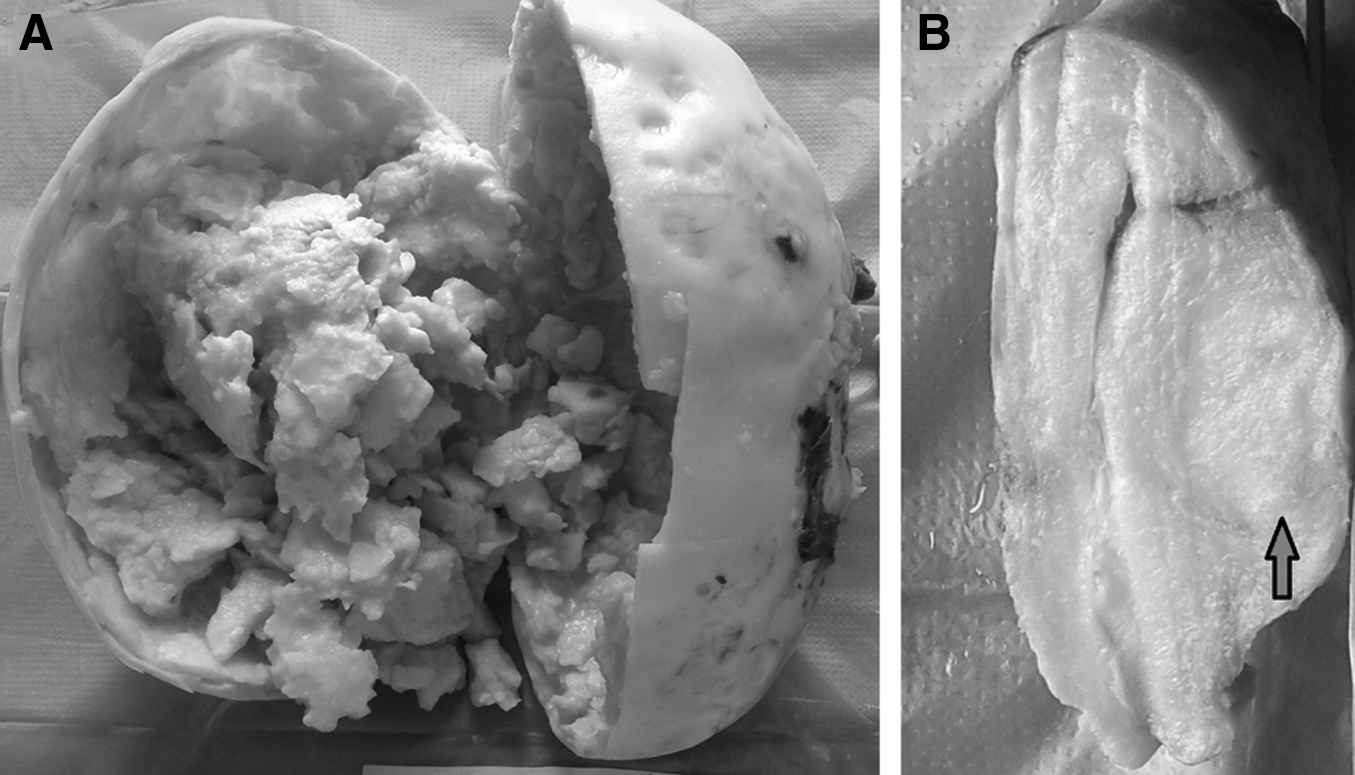
The excised mass was submitted for histopathologic examination. On gross examination, the uterus and cervix measured 7.5 × 6 × 2 cm. The left ovary measured 3 × 2 × 0.5 cm and the left fallopian tube measured 6 × 0.5 cm. The right ovary was enlarged and measured 17 × 1 4 × 10 cm. The right fallopian tube was stretched over the right ovary and measured 9 × 1 cm, and appeared to be grossly unremarkable. The enlarged right ovary was cystic and filled with yellowish thick material, with the wall thickness of the ovarian cyst varying from 0.8 to 2.5 cm (Fig. 1A). In places, the ovarian surface was indurated; however, no breech of the ovarian capsule was seen. On cutting the uterus, a well-delineated soft-to-firm, grayish–yellow tumor area was identified measuring 2 × 1.5 cm. This was limited within the myometrium and spared the endometrial cavity (Fig. 1B). The uterine serosa was intact and free from tumor deposits grossly.
Results
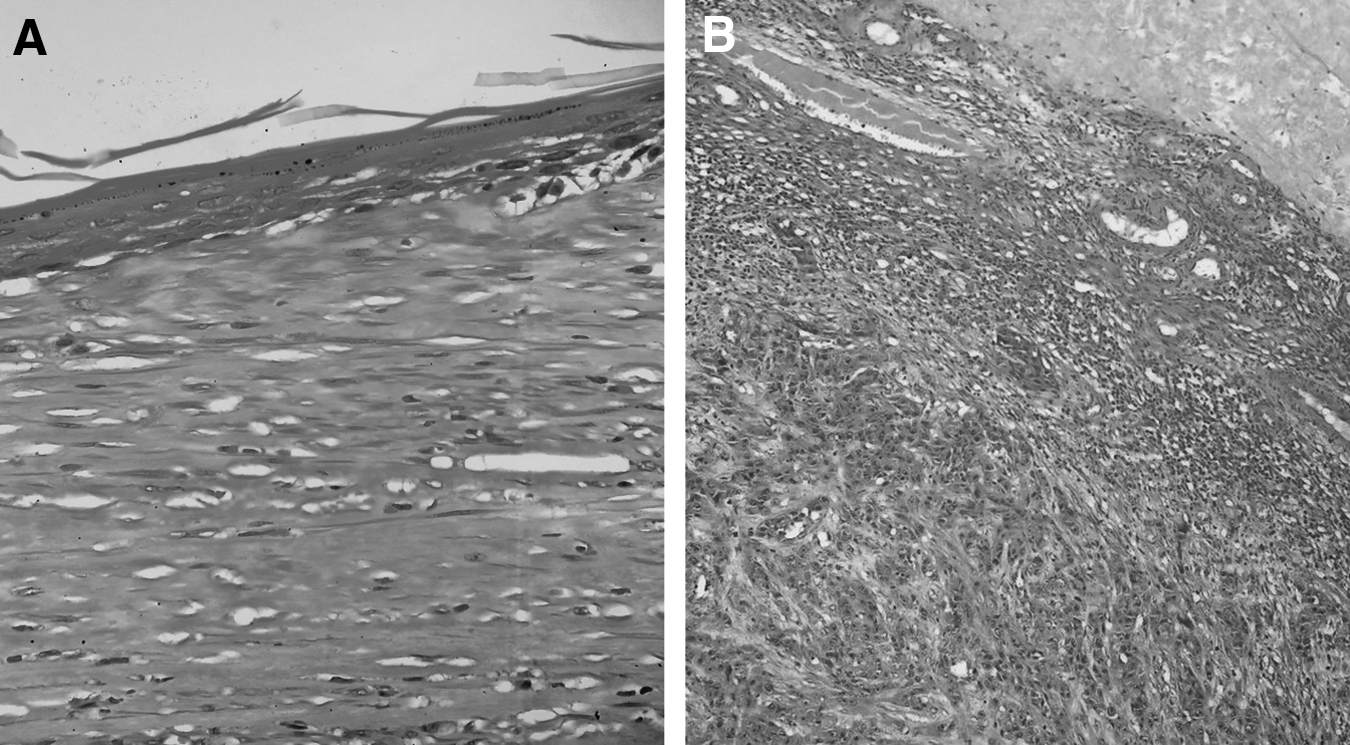
On light microscopy, a section from the thickened area of the ovarian cyst wall showed a tumor comprised of infiltrating nests and islands of malignant squamous epithelial cells with moderate pleomorphism and intercellular cytoplasmic keratinization and extracellular keratin pearls (Fig. 2). A section from the remaining cyst wall showed a lining of stratified squamous epithelium only (Fig. 3A). Adnexal structures; hair follicles; or mesodermal, endodermal, or neural components were not found even on extensive grossing. Sections from the tumor area in the uterus showed well-differentiated SCC involving the outer one-third of the myometrium (Fig. 3B). The tumor did not involve the endometrial cavity, uterine cervix, bilateral fallopian tubes, and the left ovary. All of the resected tumor margins were free of SCC. Hence, the diagnosis of well-differentiated SCC originating from the epidermoid cyst of the ovary and metastasizing to the uterus was made.
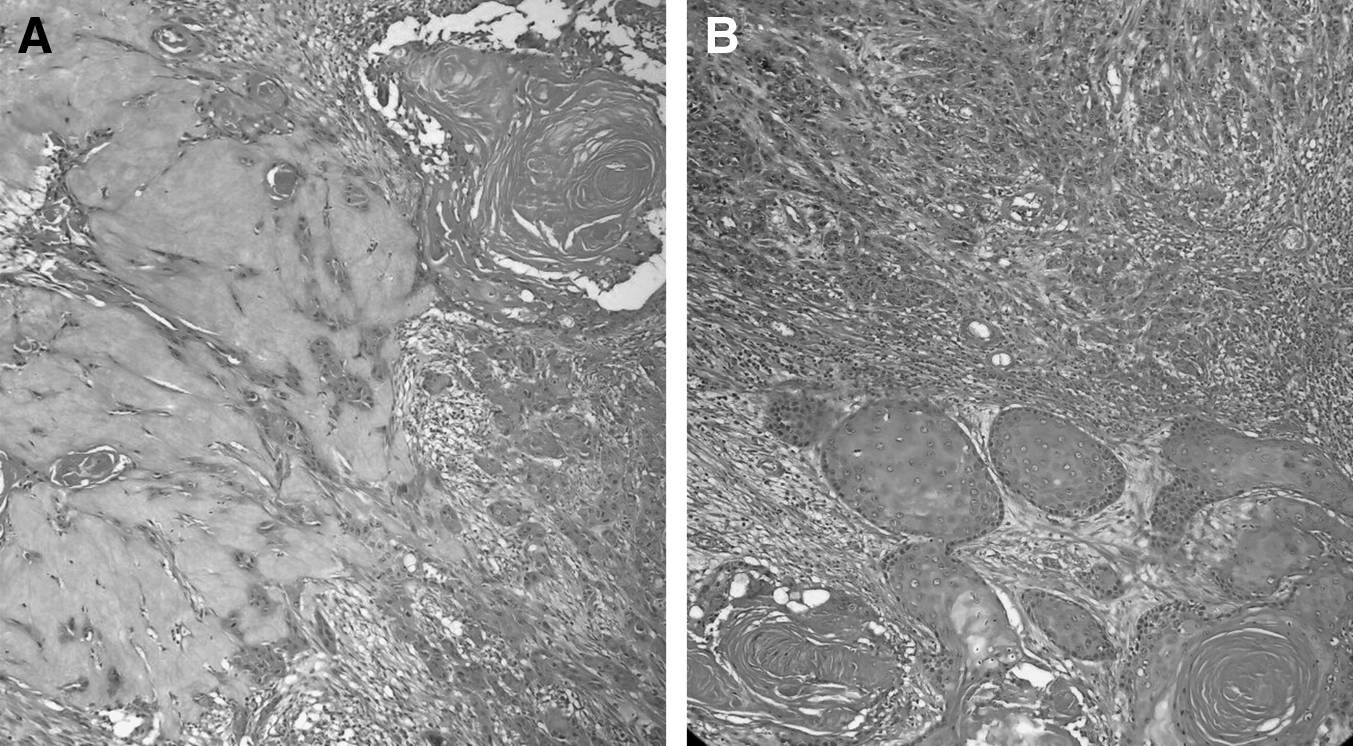
Photomicrographs showing tumor comprised of infiltrating nests and islands of malignant squamous epithelial cells with moderate pleomorphism and intercellular cytoplasmic keratinisation, and extracellular keratin pearls. Hematoxylin and eosin,
Discussion
Epidermoid cysts of the ovary are rare, and benign lesions are filled with flakes of keratin and are lined exclusively by mature stratified squamous epithelium. Epidermoid cysts differ from mature cystic teratomas of the ovary by the absence of skin adnexae and other tissues after thorough sampling. The possibility that some of these lesions are actually mature cystic teratomas in which the skin adnexal components were missed or absent (mature monodermal teratomas) cannot be totally discounted. 7 Most cases in the literature have been incidental findings in hysterectomy specimens.
An epidermoid cyst developing into SCC has not been reported in the literature. Sharma et al. reported a case of a giant epidermoid cyst measuring 17 × 10 × 10 cm in a postmenopausal female. No malignant foci was seen in that case. 6 Pins et al., in 1996, reported 11 cases of pure SCC in ovaries; however, origin from an epidermoid cyst was not seen in any of these cases. 2 Three of the cases were associated with cervical SCC in situ. These cases were categorized within the new World Health Organization category of SCC in surface epithelial–stromal tumors. 2
The histogenesis of epidermoid cysts has not been described completely. The earliest cases were reported by Nogales and Silverberg in 1976, and they suggested that metaplasia of the coelomic surface epithelium of the ovary was involved in the histogenesis of these lesions. 8 Young et al. described 3 cases in 1980 and, after making a comparative study of these lesions, the presence of Walthard nests and epithelial components of Brenner tumors suggested that these cysts originated from epithelial-cell nests of the type encountered in Brenner tumors. 9 Fan et al., in their series of 8 cases, suggested that ovarian epidermoid cysts represented monodermal and highly differentiated teratomas and should be classified as such. 10 These researchers also believed that epidermoid cysts of the ovary were not as rare as the literature suggested and that some were probably misdiagnosed as dermoid cysts.
Epidermoid cysts associated with surface epithelial tumors, germ-cell tumors, and monodermal teratomas have been described.9–11 The current case is the first one showing an epidermoid cyst with SCC and metastasizing to the myometrium. Khedmati et al. conducted the largest clinicopathologic study on 18 cases of epidermoid cysts in comparison to 120 mature cystic teratomas in 2009. 4 These researchers had concluded that an epidermoid cysts of the ovaries, as defined by histology, comprised a heterogeneous group. Pure epidermoid cysts probably represent <1% of ovarian epithelial tumors.
In a study conducted by Chen et al., four tumor markers, SCC antigen, CA-125, CA-199, and carcinoembryonic antigen, were evaluated in patients with SCC. The researchers concluded that SCC antigen had the highest positive rate (81.3%) in patients with SCC arising from mature cystic teratomas. A lower positive rate (15%) for SCC antigen was found in nonmalignant mature cystic teratomas. 1 The SCC antigen levels increased in accordance with the International Federation of Gynaecology and Obstetrics stage severity. However, for predicting prognosis and survival rate, preoperative values of SCC antigen and CA-125 are necessary. A positive CA-125 level was found to be a more reliable marker of predicting whether or not a case of SCC will have a poor prognosis. These serum makers are valuable for obtaining preoperative diagnosis, as these tumors are missed radiologically. These marker studies are not available in the current authors' institute, so they were not performed for the current case.
Given that there is no specific symptom or sign, even in radiologic imaging, it is challenging to diagnose ovarian SCC prior to surgery, unless the tumors are in an advanced stage. Hence, postoperative histopathologic analysis becomes inevitable.
Conclusions
Epidermoid cysts can transform into SCC, and such a diagnosis should only be made only after extensive sampling has been done. The presence of hair follicles and sebaceous glands should be ruled out, to differentiate the mass from a dermoid cyst or monodermal teratoma. Preoperative diagnosis becomes difficult due to lack of specific signs, symptoms, and imaging findings. Hence, diagnosis according to histopathology is essential.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.