
Abstract
Abstract
Objective:
The aim of this research was to determine the impact of laparoscopic ovarian cystectomy on ovarian reserve.
Materials and Methods:
This was a prospective observational study carried out on 15 women, 15–40 years of age, who underwent laparoscopic ovarian cystectomy for symptomatic benign ovarian cysts of size >7 cm in the Department of Obstetrics and Gynaecology at Pt. B.D. Sharma Postgraduate Institute of Medical Sciences, in Rohtak, Haryana, India, a tertiary care center of north India. Bipolar electrocoagulation was used for hemostasis on the ovarian bed during surgery. Serum anti-Müllerian hormone (AMH) was measured 1 day prior to surgery (D0), on postoperative day 7 (D7), and on day 90 (D90), using an enzyme-linked immunosorbent assay. The data were analyzed using SPSS 16.
Results:
The mean age in the study was 27 ± 6.92 years and 13 (86.66%) women were under age 35. Three (20%) women had presented with infertility, and the remaining (80%) with dull abdominal pain. A declining trend of mean AMH levels with increasing age and cyst size was noted in the study. Nine (60%) women had AMH values between 2.1 and 5 ng/mL preoperatively, while 6 (40%) had values between 5.1 and 9 ng/mL. However, on D7, 9 women (60%) had values between 1 and 3 ng/mL on D7, suggesting a decline in AMH values in some women who had higher levels earlier. All women in the study had preoperative AMH values >2 ng/mL, indicating optimal ovarian reserve, while 5 (33.33%) women on D7 and 2 (13.33%) women on D90 had AMH levels <2 ng/mL, suggesting some recovery in 3 cases. A significant fall in mean AMH levels was seen between D0 and D7 (38.78%; p < 0.001) and between D0 and D90 (46.73%, p < 0.001) in the study.
Conclusions:
Laparoscopic ovarian cystectomy using bipolar coagulation causes a significant continuous decline in ovarian reserve as measured by serum AMH. (J GYNECOL SURG 33:129)
Introduction
T
Benign cysts of the ovary may be functional, corpus luteal, hemorrhagic, teratoma, cystadenoma, or endometrioid, and can present with infertility, pain in the abdomen or pelvis, and/or pressure symptoms. Large ovarian cysts are commonly managed by cystectomy, wherein the entire cyst wall is removed leaving behind the normal ovary. Removal of the cyst wall from the ovary may result in reduction in the ovarian reserve consequent upon inadvertent removal of healthy ovarian tissue or vascular compromise or both. 3 During laparoscopic cystectomy, hemostasis is commonly achieved by using some form of coagulation. The present study was conducted to evaluate the effect of laparoscopic ovarian cystectomy on serum AMH levels and hence on the ovarian reserve.
Materials and Methods
Patients
This prospective study was conducted on 15 women aged 15–40 who were diagnosed with benign ovarian cysts of 7 cm or more in size at Pt. B.D. Sharma Postgraduate Institute of Medical Sciences, in Rohtak, Haryana, India, a tertiary care center of north India. Women with bilateral cysts, malignant ovarian cysts, or inflammatory tubo-ovarian masses, and women with histories of previous ovarian surgeries were excluded from the study.
Tests and procedures
After each patient gave her informed written consent, a detailed history—including the age of the patient, her complaints, obstetric history, and/or past history of any systemic/medical disorder—was taken. General physical, systemic and gynecological examinations were carried out, including abdominal, speculum, and bimanual digital examinations for size of the uterus, and size, consistency and mobility of the adnexal mass. Hemoglobin estimation; bleeding time; clotting time; blood group; serologic tests for human immunodeficiency virus, hepatitis B and C; chest X-ray; and electrocardiography were also carried out. Each woman underwent ultrasonography for evaluation of her uterus and size and contents of the adnexal mass. Estimation of AMH was done 1 day prior to surgery (D0) and repeated on postoperative day 7 (D7) and day 90 (D90) by enzyme-linked immunosorbent assay (ELISA), with a commercial ELISA kit that uses anti-AMH antibodies to bind to AMH. According to the manufacturer's protocol the detection limit of AMH was 0.006 ng/mL and the intra-assay variation of coefficients were <10%. Serum AMH values between 2 and 6.8 ng/mL were considered to be in normal range, indicating optimal ovarian reserve, and values <2ng/mL were considered to be indicative of poor ovarian reserve.
Three-port conventional closed laparoscopic cystectomy was performed on each patient by insertion of an 11-mm trocar through a sub-umbilical transverse incision followed by introduction of a 10-mm laparoscope after creating a pneumoperitoneum, and two 5-mm ancillary ports were also placed. After inspection of the peritoneal cavity, cystectomy was performed by enucleating the cyst from the ovarian bed, taking care to avoid spillage of the cyst's contents (Fig. 1). Bipolar electrocoagulation was used for hemostasis on the ovarian parenchyma, being careful not to damage the ovarian hilus during the procedure. The cyst wall was removed from the abdomen by an endobag, and all obtained specimens were sent for histopathology. The ovary was left unsutured after ensuring hemostasis. The patient's postoperative course was monitored and she was discharged after 24 hours in the absence of any complications.
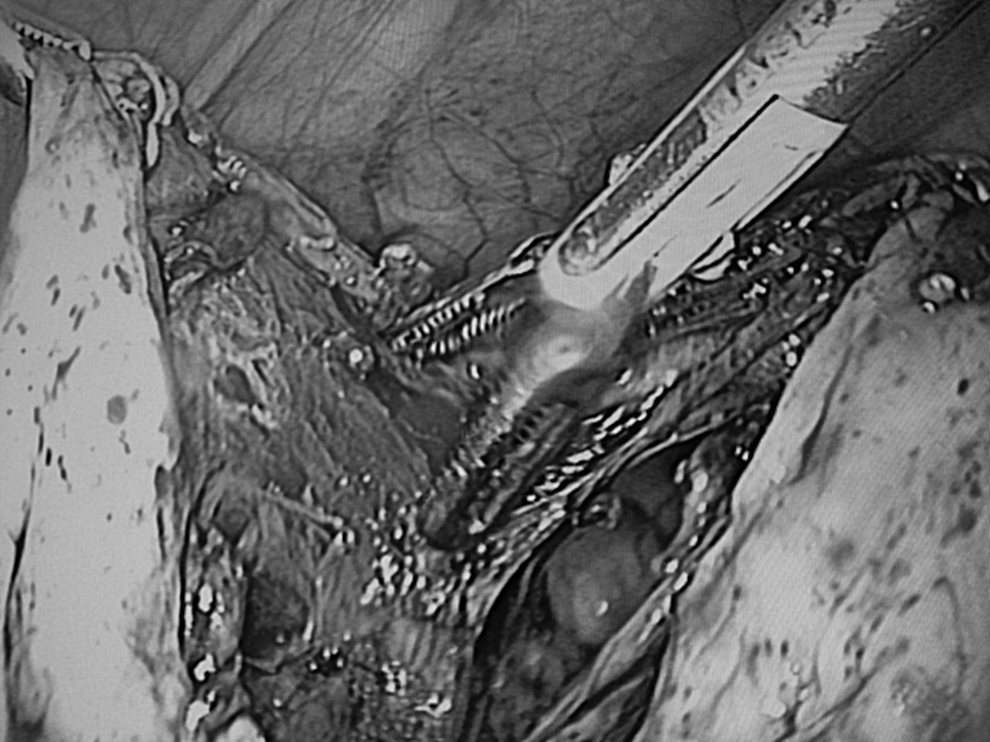
Intraoperative picture showing bipolar electrocoagulation of ovarian bed during laparoscopic cystectomy.
All women were called for follow-up on postoperative D7 and D 90 when blood samples were collected for AMH estimation and complaints, if any, were addressed.
Statistics
The data on these patients were analyzed statistically using SPSS 16 software.
Results
All of the women in the study were between ages 16 and 40, with a mean age of 27 ± 6.92 years. Thirteen (86.66%) women were younger than age 35. Eleven (73.33%) women were educated up to graduation level and only 4 (26.66%) women in the study group were employed, with the remaining being homemakers. Ten (66.66%) women were married and 7 (46.66%) were parous. Three (20%) women had presented with infertility, and the remaining (80%) women presented with dull abdominal pain. Table 1 shows mean AMH levels in the study, according to age and size of the cysts as measured on ultrasonography. The preoperative size of ovarian cysts on ultrasonography ranged between 7 and 14 cm, with the mean size being 9.25 ± 2.25 cm, and the contents were clear (serous) in 10 (66.66%), echogenic in 1(6.66%), and variable in 4 (26.66%) women. A declining trend of mean AMH levels with increasing age and cyst size was evident, as shown in Table 1.
AMH, anti-Müllerian hormone, SD, standard deviation.
Table 2 shows the mean AMH values on D0, D7, and D90 in the study. It was evident, as shown in Table 2, that 9 of 15 women (60%) had AMH values between 2.1 and 5 ng/mL preoperatively, and only 6 women (40%) had values between 5.1 and 9 ng/mL. However, on D7, 9 women (60%) had values between 1 and 3 ng/mL, suggesting a decline in AMH values in some women who earlier had higher levels. Similarly, 3 women had D0 AMH values >7.1 ng/mL but none had values in this range after surgery. All the patients had AMH values up to 5.3 ng/mL on D 90. This is in comparison to the highest AMH values of 8.1 ng/mL and 6.6 ng/mL on D0 and D7, respectively. In terms of ovarian reserve, all women in the study had preoperative AMH values >2 ng/mL, indicating optimal ovarian reserve, while 5 (33.33%) women on D7 and 2 (13.33%) on D90 had AMH levels <2 ng/mL, suggesting some recovery in 3 cases.
AMH, anti-Müllerian hormone, SD, standard deviation.
Table 3 shows the decline in AMH levels in the study. A significant fall in mean AMH levels between D0 and D7 and between D0 and D90 was evident.
AMH, anti-Müllerian hormone, SD, standard deviation.
Histologically, there were 9 cystadenomas, 4 benign cystic teratomas, and 2 endometriomas in the study. The mean preoperative size of the 2 endometrioid cysts was 8.8 cm, in comparison to 9.1 cm for dermoids and 11.7 cm for cystadenomas. The women with endometriotic cysts were aged 23 and 28. Table 4 shows the preoperative mean AMH levels in various histopathologic variants of ovarian cysts.
AMH, anti-Müllerian hormone, SD, standard deviation.
Discussion
A decline in ovarian reserve with advancing age that was evident in this study is believed to be the result of a progressively depleting pool of follicles with each menstrual cycle and decreased gene expression of proteins involved in DNA repair by homologous recombination, such as BRCA 1, MRE11, Rad51, and ATM. 4 A simple unilocular cyst was the most common type of ovarian cyst in the study. Histologically, dermoids and endometrioid varieties were the commoner variants. Similar trends in incidence were reported by Amooee et al. in their study on 60 women. 5
The present study indicated a significant reduction in ovarian reserve after laparoscopic ovarian cystectomy by D7, suggesting a steep fall in the first postoperative week, which continued further up to 3 months, albeit at a much slower rate. Most other researchers have documented a 32%–53% decline in AMH values after 3 months post laparoscopic cystectomy.6–9 Amooee et al. showed a decline in AMH by 45%–58% at 1 month, followed by starting of a phase of recovery at 3 months, wherein a 62%–67% recovery was noted. 5 However, the AMH levels never reached baseline levels in any study. Zaitoun et al. demonstrated a significant continuous decline in their laparoscopy group even at 18 months postoperatively and concluded that there was more damage to ovarian reserve caused by laparoscopy, damage that continues for as long as 18 months. 10
Several possible mechanisms may underlie the reduction of ovarian reserve after ovarian cystectomy.
First, inadvertent removal of variable amount of functional ovarian tissue occurs at cystectomy, which may be the primary cause of the adverse impact on the follicular function of the remaining ovary.
Second, the size of the cyst and effect on the contralateral ovary by similar cystic development in cases of bilaterality may also affect residual AMH values. This effect may be more pronounced in endometriotic cysts, which tend to have a pseudocapsule, and enucleation/stripping the lining in such cases usually leaves behind more bleeders.11,12
Third, direct damage from electrosurgical coagulation for hemostasis may contribute to the destruction of functional tissue around the vessels. In bipolar coagulation, the tissue between the tips of the prongs of the bipolar instrument is subjected to an electrical current. The spread of current and heat with bipolar is less than for a monopolar current; however, the thermal impact on the surrounding cells cannot be considered negligible. Intracellular proteins have a very narrow temperature window for optimal function, and an unquantified temporary or permanent functional impairment can result. In addition, the ultimate impact would depend on the extent of thermal injury (i.e., the number of electrical applications carried out and the areas coagulated are also likely to impact the residual function).13,14 Proximity to the ovarian hilus can be another factor that could affect the ultimate ischemic impact on the ovarian parenchyma but this has not been evaluated objectively so far. Apart from the direct electrical damage, inflammation-mediated injury may compromise the secretory function of a variable number of surrounding follicles. 15
The steep fall in the ovarian reserve in the first week suggests that most functional damage occurs during this time, and the timing of this manifestation supports an ischemic etiology. Hence, measures to minimize loss of functional ovarian tissue and ischemic damage to perivascular follicles would help conserve the ovarian reserve. The current authors suggest that a linear incision on the cyst wall at enucleation should be preferred over a circular incision all around the cyst, which tends to a remove larger amount of ovarian tissue from over the cyst. In addition, precise localization of the bleeder and use of a fine-tip bipolar instrument can help reduce damage to tissues around the vessels in the ovarian bed. Care should be taken to avoid damage to hilar vessels, although the location of the cyst would determine which feeding vessels need occlusion.
Low-dose aspirin has been shown to significantly improve ovarian responsiveness and ovarian blood flow velocity, number of oocytes retrieved, serum E2 levels, and implantation and pregnancy rates in women undergoing in-vitro fertilization. 16 However, there are no studies to suggest that low-dose aspirin is effective for retaining ovarian reserve after cystectomy. The quest for better energy sources for laparoscopy, ensuring minimal adjacent impact, continues.
Conclusions
Laparoscopic ovarian cystectomy using bipolar coagulation causes a significant and continuous decline in the ovarian reserve as measured by serum AMH. However, the present study was limited by the number of participants. More large-scale randomized trials on conservation of ovarian reserve in various benign ovarian cysts are suggested.
Footnotes
Author Disclosure Statement
There are no competing financial interests, actual or potential, for any of the authors of this article.