
Abstract
Abstract
Background:
In current practice, abdominal pregnancy is rarely encountered. It seems to be more common in disadvantaged areas or in areas where there is insufficient prenatal follow-up for the population. Abdominal pregnancies are often encountered in advanced stages or at term. The resulting consequences are related to late diagnosis and high mortality and maternal–fetal morbidity. The types discovered early are classically terminated; however advanced cases comprise a topic of discussion.
Case:
A 35-year-old patient, primigravida, was being monitored in a secondary-level healthcare center. Her abdominal pregnancy was discovered by routine ultrasound (US) at 16 weeks, and close follow-up was planned. She was admitted to a hospital when the pregnancy reached 35 weeks for minimal bleeding, with no fetal movement and cardiac activity. The results of the US and computed tomography scanning showed oligohydramnios, a still fetus, in a transverse position, with overlapping bones of the skull. A laparotomy and an extraction of the fetus with the placenta as a whole were carried out with an uneventful follow-up period.
Results:
The postoperative events were simple and she had a postoperative hemoglobin level of 8 g/L. No complaints were noted during her follow-up.
Conclusions:
Prenatal follow-up by quality US is essential for early diagnosis of abdominal pregnancy. The prognosis of such pregnancies diagnosed early remains unpredictable, with reduced chances of success.
Introduction
A
Abdominal pregnancy is associated with a high fetal morbidity and mortality rate. Malformations are observed in 20%–40% of cases, and fetal mortality can occur in 95% of the cases.1,3 Maternal complications are frequent, dominated by a hemoperitonium, caused by spontaneous separation of the placenta, and infection. The placenta may also be implanted in neighboring vital organs requiring an adhesiolysis, with a high risk of massive intraoperative bleeding or an intestinal fistula. Increasingly, the option to leave the placenta on-site and ensure hemostasis is chosen, and a follow-up of the placental evolution is maintained in the postoperative period. The forms of abdominal pregnancy that are diagnosed early are classically indications to terminate these pregnancies. However, advanced forms comprise a topic of discussion.
This article reports on a case of abdominal pregnancy at 36 weeks and discusses the epidemiologic and clinical aspects, as well as treatment options in disadvantaged areas.
Case
A 35-year-old illiterate patient, without any particular significant medical history, was monitored at a secondary healthcare center during her pregnancy. She was primigravida, had no complaints, and had 2 prior prenatal visits. An US performed at 16 weeks of amenorrhea had revealed an abdominal pregnancy for which surveillance and maturation had been decided.
She was admitted at 36 weeks of amenorrhea, with vague abdominal pains and minimal bleeding. She signaled that she would not be able to continue with prenatal visits because of financial difficulties.
On examination, the patient was found in good general condition; her American Society of Anesthesiologists status was 1, with normal mucous membranes. Her blood pressure was 140/90 mm Hg, her pulse was 95 beats/minute, and her temperature was 37.5°C. An abdominal right lateralized, molasse, mobile, painless mass was noted. On vaginal examination, the uterus was palpated and had a normal gynecologic size; and the cervix was of medium length, anterior, and closed.
A complete blood count showed a hemoglobin level of 10 g/dL, white blood cells at 7540/L, and a platelet count of 132,000. The prothrombin rate was at 73%, international normalized ration was at 1.31, and blood glucose was at 0.70 mg/L.
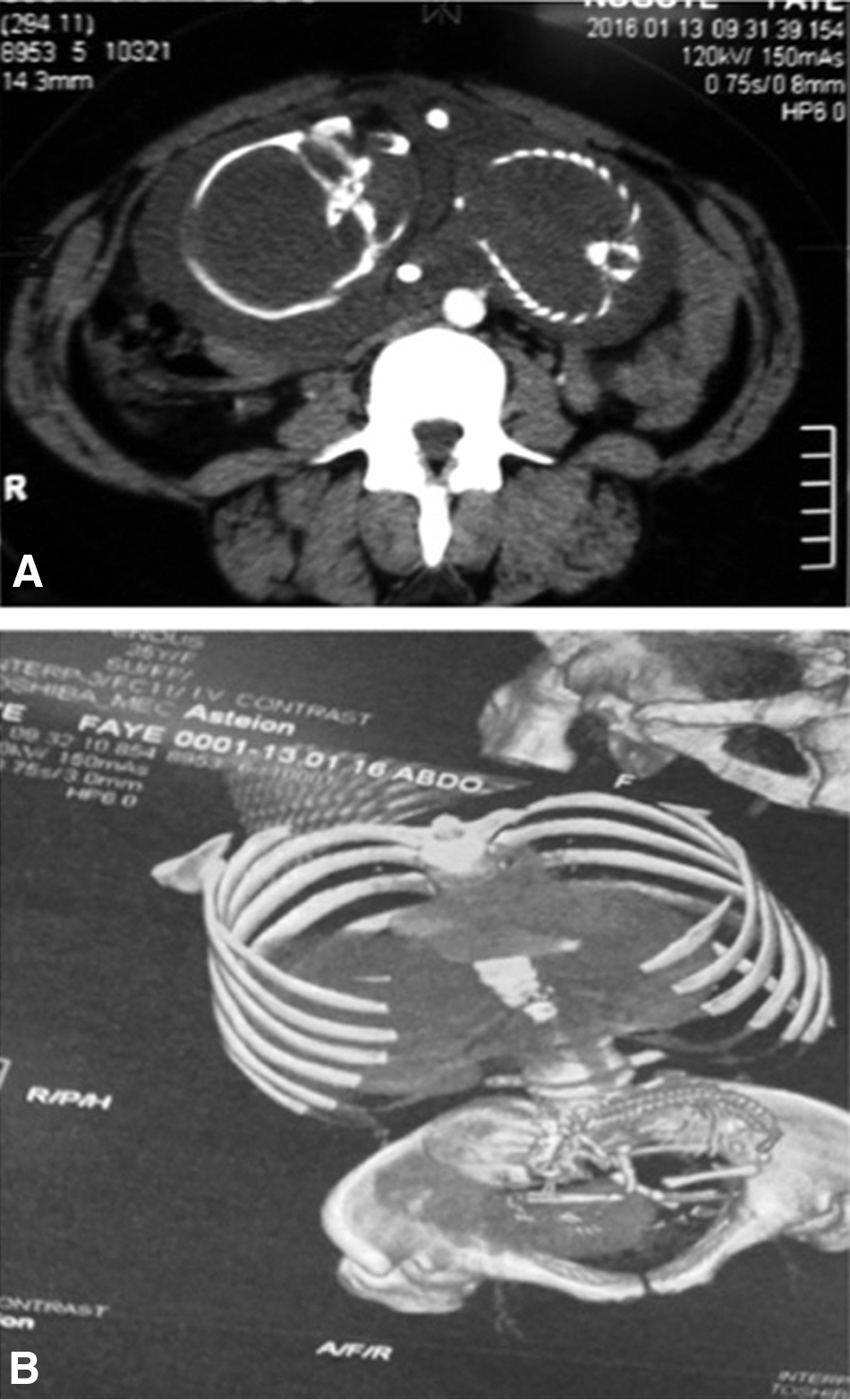
An US showed an empty uterus, an abdominally situated fetus in a transverse position, with a well-visualized placenta and separated from the intestines by an interface membrane. The fetus was inactive, with no cardiac activity, and had overlapping skull bones and a detached scalp. Abdominal computed tomography (CT) scan findings were identical to those of the US and did not show any adhesions to vital intraperitoneal organs (Fig. 1).
(
A median laparotomy revealed an abdominal pregnancy with a placenta implanted on the right ovary and fallopian tube from where it derived its vascularity (Fig. 2). The placenta adhered to the anterolateral abdominal wall, the small intestine, sigmoid colon, and the pelvic wall. The uterus consistency was slightly molasse hypertrophied (Fig. 3). Adhesiolysis was performed with a right salpingectomy taking the membrane along without opening the placenta (Fig. 4). The entire placenta was removed, and hemostasis controlled without drainage. It contained a fetus of 900 g (Fig. 5).

(

Normal uterus, with placenta inserted on the ovary at the right fallopian tube

Intact placenta.

Fetus and blackish brown amniotic fluid.
Results
The postoperative events were simple with postoperative hemoglobin of 8 g/L. No complaints were noted during the follow-up.
Discussion
Abdominal pregnancy remains extremely rare in current practice but is the only form of ectopic pregnancy that can eventually evolve to term. However, tubal pregnancy remains the most common ectopic pregnancy type and accounts for 95% of cases. In 5% of cases, the fertilized egg can be implanted on the cervix or interstitial and uterine horn; attached to a previous Cesarean-section scar; found at the ovarian level; and exceptionally in an intraperitoneal area.4,5 The incidence rate of abdominal pregnancy is diverse; it varies from 1/10,000 to 1/30,000, depending on the regions in which it occurs. It is estimated at 1/10,000 in developed countries and 3.4/10,000 in developing countries.2,3,6,7 Prenatal services for the population remain a major public health problem in sub-Saharan Africa. Remoteness and difficulties regarding access to healthcare institutions, combined with poor attendance and quality of care, reveal the historical clinical pictures being seen. Abdominal pregnancies are classically seen in their advanced forms, or are discovered fortuitously at term or perioperatively during a Cesarean section, as reported by Gueye in the same region of the world. 8
Abdominal pregnancy can be the result of primary embryologic implantation in the peritoneal cavity, or, in most cases, as the result of a spontaneous tubal–abdominal migration or a rupture of the fallopian tube. Migration may also occur through a dehiscence of a hysterotomy. As with extrauterine pregnancy, the risk factors include infertility, chlamydia infection, pelviperitonitis, endometriosis, tubal malformations, intrauterine devices, uterine aspirations, and in-vitro fertilization. Tubal sequelae of infectious origin are the most common factors in these regions of the world.
Abdominal pregnancy can remain asymptomatic and be discovered fortuitously in the second or third quarter of a pregnancy.2,4,8 Vague abdominal pain and minimal bleeding are frequently described in the first few months without real specificity. Later, other small signs must raise suspicion about the possibility of abdominal localization of the pregnancy. This would include painful fetal movements felt under the skin; the superficial fetal skeleton, easily palpable under a loose abdominal wall; and a platelike fixed uterine cervix under the symphysis pubic. However, no symptoms in the current patient were reported except for abdominal pain “waves” and minimal bleeding.
Diagnosis rests on US, which shows an empty uterus, extrauterine placental insertion, the fetus in a transverse position, an absence of myometrium around the fetus or between the placenta and the bladder wall; and oligohydramnios, with the fetus attached to the abdominal wall.9,10 US is also used to evaluate fetal vitality and to search for malformations. However, the ultrasound misses showing the intraperitoneal position in 25% of cases.9,11–13 In cases of doubt, MRI is a precious and precise diagnostic aid for determining the intraperitoneal position, exact placental implantation site, and relationship with neighboring organs.14,15 In the current authors' case, absence of fetal activity led to the use of a CT scan, which produced the same findings.
Management depends on the earliness or lateness of the diagnosis and the state of the fetus at diagnosis time. Management also takes into account risks of malformation and maternal–fetal mortality. Fetal malformations can reach up to 40%. The malformations are often skeletal in nature and are associated with oligohydramnios. They are characterized by cranial and facial asymmetry; neck, knee, elbow, and foot deformations; torticollis; and varus equine.2,16 Congenital malformations are rare. Postoperative death caused by distress is frequent and associated with the malformations and pulmonary hypoplasia.8,13
Maternal mortality can reach 15%–18% of cases, dominated by the risk of pre- or postoperative hemorrhage, severe infection, fistula, occlusion, and coagulopathy.1,2,4,12,17 Before 20 weeks, it is classic to propose a laparotomy and extraction.17,18 For the current patient, the decision to prolong the pregnancy by the secondary-center team certainly reduced chances of success. Indeed, this situation requires hospitalization and follow-up monitoring by a multidisciplinary team.13,12,18
The advanced forms, near-term with a live fetus, pose a serious dilemma between performing an immediate laparotomy to limit the high maternal–fetal mortality risk or prolonging the pregnancy at 34 weeks with a planned laparotomy. The choice also involves accounting for the medical environment and clinical criteria as recommended by Martin and McCaul, who proposed 8 criteria: (1) living fetus; (2) lack of severe congenital defects; (3) lack of maternal and fetal distress; (4) low placental implantation in the abdomen; (5) enough amniotic fluid volume with intact membranes; (6) good fetal condition; (7) hospitalization in an equipped maternity facility; and (8) a well-informed patient who consents. 19
During extraction, placental bleeding risks are real. In the current patient, a relatively easy abruption was obtained and complete extraction was carried out with control of hemostasis. Abandonment of the placenta in-situ is highly recommended today along with involution-controlled imagery and a regular dosage of ß–human chorionic gonadotropin.4,8,16
Conclusions
Early diagnosis of abdominal pregnancy is essential to reduce high morbidity and maternal–fetal mortality. This approach is based on regular prenatal visits and using quality US. The therapeutic attitude regarding early forms is commonly in favor of laparotomy. Surveillance in disadvantaged areas remains difficult with reduced chances of success.
Footnotes
Acknowledgments
The authors thank Adamson Phiri, MD, for helpful criticism, advice, and assistance with revising and translating the manuscript for this article.
Author Disclosure Statement
The authors report no conflicts of interest.