
Abstract
Abstract
Background:
The occurrence of simultaneous ectopic pregnancies in two extrauterine locations is rare, particularly in spontaneous pregnancies.
Case:
This article describes the case of a 32-year-old woman who presented with persistently elevated β-hCG levels after a salpingectomy for a left ectopic tubal pregnancy.
Results:
Follow-up elevated β-hCG levels led to the discovery of a simultaneous right tubal ectopic pregnancy.
Conclusions:
Bilateral ectopic pregnancy is rare but must be suspected when β-hCG is elevated after treatment of an ectopic pregnancy. β-hCG follow-up can be helpful, even if chorionic villi are present in the initial surgical specimen. (J GYNECOL SURG 33:202)
Introduction
I
In the absence of ovulation induction, bilateral ectopic pregnancy is an extremely rare occurrence. Its estimated incidence is 1 in 725 to 1 in 1580 of all ectopic pregnancies.2–4 This article reports on a case of a spontaneous bilateral ectopic pregnancy that was only recognized after a patient had persistent elevated β–human chorionic gonadotropin (β-hCG) levels after a salpingectomy.
Case
A 32-year-old, gravida 4, para 3003, female presented on December 21, 2015, to an emergency department (ED) with a 1-day history of sharp, lower-left quadrant pain. The patient's last menstrual period prior to presentation was November 8, 2015, and she had a positive home urine pregnancy test taken the day prior to presentation. She denied having vaginal bleeding or any other complaints at the time. She also denied having any medical, surgical, social, or gynecologic history. She had a history of 3 spontaneous vaginal deliveries. She was not taking any medication or using contraception, as she desired pregnancy. In the ED, the patient underwent a pelvic ultrasound (US) that showed a left ectopic pregnancy consistent with 5 weeks and 1 day (gestational sac), with the presence of a yolk sac; no evidence of intrauterine pregnancy; and a normal-appearing right adnexa. Her β-hCG was 1388 mIU/mL. The patient underwent a laparoscopic left salpingectomy on the same day. Surgical findings revealed a small hemoperitoneum and thin filmy pelvic adhesions on the uterus and left fallopian tube. The right fallopian tube appeared to be normal and intact, with no bleeding observed from the fimbriated end of the tube. The patient was discharged a few hours after surgery. She was given RhoGAM® for an O-negative blood type prior to discharge.
The pathology from the salpingectomy confirmed the presence of chorionic villi in the fallopian tube, consistent with a left ectopic pregnancy.
Results
The patient was scheduled to return to the clinic within the week for a postoperative check; however, due to holiday scheduling conflicts, as well as difficulty with contacting her, she was not able to return until 19 days after her surgery (January 8, 2016). At that time, her β-hCG was retested. The patient denied engaging in any coital activity since her surgery. Her β-hCG had decreased from 1388 mIU/mL (prior to surgery) to 1010 mIU/mL. There was concern about this persistently elevated β-hCG; thus, the patient was then contacted to return for another confirmatory level test to ensure that this value was not due to laboratory error. She returned to the laboratory 1 week later, on January 15, 2016, when her β-hCG was 1459. Due to this increase in β-hCG, she was contacted to return for evaluation. The patient, however, returned to the laboratory only on January 19, 2016 and left without further US evaluation; her β-hCG was 1455. The patient was contacted the next day with explicit instructions to come to the emergency room for evaluation including US testing. She presented to the ED on January 22, 2016, when her β-hCG was 1169.
At that time, the patient underwent a repeat pelvic US, which showed a 1.4-cm right ectopic pregnancy and no intrauterine pregnancy (Fig. 1). The patient opted for medical therapy, and she received methotrexate. Her β-hCG was followed on days 4 and 7 and showed an appropriate decrease (> 15%) from 941 to 691. Her β-hCG continued to decrease and was 2 mIU/mL on February 23, 2016, 32 days after methotrexate administration.
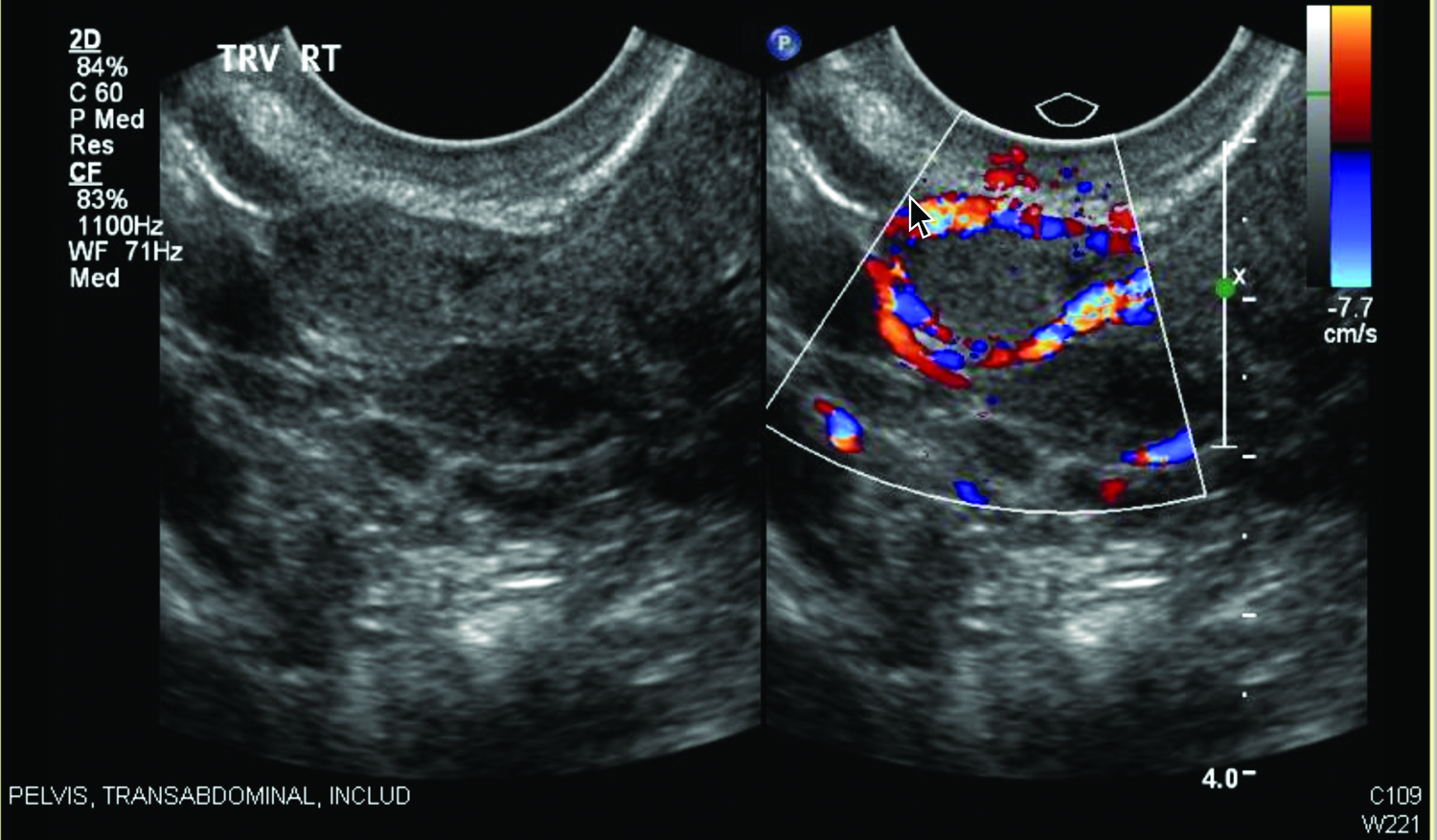
Anterior to the right ovary in the region of the distal right fallopian tube, a 1.4 × 0.7 × 1–cm homogeneous soft tissue structure (left) with a circumferential “ring-of-fire” (right) on seen on color Doppler, indicating a right ectopic pregnancy. Color images available online at www.liebertpub.com/gyn
Discussion
It is known that the incidence of ectopic pregnancies had increased to reach a plateau of 2 in 100 pregnancies in the early 1990s. 5 This has mostly been associated with the increased incidence of pelvic inflammatory disease. 6 In the absence of ovulation induction, bilateral tubal pregnancy is the rarest form of ectopic pregnancy. Despite ovulation induction, theoretically increasing the risk of multiple ovulations and consequently the risk of bilateral ectopic pregnancy, the latter can still occur in a normal cycle. According to Brewer and Jones in 1941, and Ritchie in 1985, ovulation from both ovaries has been reported to be in the frequency of 5%–10% per menstrual cycle.7,8 According to the Centers for Disease Control and Prevention, there are ∼6 million pregnancies annually 9 and only 1 in 400,000 of them are spontaneous bilateral tubal pregnancies. 10
Bilateral tubal ectopic pregnancy is usually diagnosed intraoperatively.2,11 One report described a patient who underwent serial salpingectomies separated by a few weeks because of a ruptured ectopic pregnancy that had occurred after she had been treated surgically for a first tubal pregnancy, 12 which emphasizes how important it is to identify and examine both fallopian tubes during surgery.
Preoperative diagnosis would be ideal. Advances in color Doppler techniques have increased the sensitivity of transvaginal US, which should increase the likelihood of detecting a bilateral ectopic pregnancy before a surgical procedure, 13 particularly if this kind of pregnancy is looked for. After treatment of ectopic pregnancy, the current authors think it is important to continue to follow β-hCG levels immediately postoperatively until these levels go down to a negative value. A plateau or increasing level of β-hCG signifies that trophoblastic disease is still present and that further evaluation should be performed, even in patients with confirmatory pathology results from their procedures (usually chorionic villi). 14
Conclusions
It is important to be aware of the possibility of bilateral tubal ectopic pregnancies, in spontaneous pregnancies as well as in those after ovulation induction, particularly if there is persistently elevated β-hCG after therapy.
Footnotes
Author Disclosure Statement
There was no financial support for the study. No funding was received for this work. There are no conflicts of interest.