
Abstract
Abstract
Objective:
A magnetic resonance imaging (MRI)–based three-dimensional (3D) reconstruction of uteri anatomy was applied to determine if this reconstruction had diagnostic accuracy and an effect on planning and performance of surgical procedures for uterine fibromatosis.
Materials and Methods:
Patient-specific 3D models of the uteri of 18 women with symptomatic fibromatosis selected for surgery were obtained from MRI images with semiautomated segmentation routines and were shown to a surgeon at the time of presurgical planning and during surgery. Diagnostic accuracy of the 3D reconstruction versus transvaginal ultrasound (TVUS) in identifying and locating the myomas was tested. The impact of the 3D modeling on the choice and the performance of surgery was compared with 30 comparable procedures for which MRI was not available.
Results:
Sensitivity of the 3D imaging system was higher than TVUS, at 97% versus 72%. Preoperative visualization of the 3D images induced the surgeon to shift from a presurgical plan of open surgery to a mini-invasive technique in 22% of patients and from total hysterectomy to myomectomy in 31% of patients.
Conclusions:
3D imaging of uteri with a MRI-based system identifies and locates myomas with high sensitivity and appears to be useful for both planning and execution of surgery. (J GYNECOL SURG 33:138)
Introduction
P
To this extent, patient-specific 3D models reconstructed from volumetric images could be helpful, given that they are visually intuitive and alleviate the challenge of mental reconstruction. 2 Current methods to achieve 3D reconstructions are based on elaboration of ultrasound (US), computerized tomography (CT) or magnetic resonance imaging (MRI) data. MRI and CT images are particularly fit to be elaborated by tools included in radiologic software. This approach allows reconstructing organs, tissues, and their lesions accurately. 3
Computer tools can be used to enhance the visual experience further, allowing a realistic representation of a patient's anatomy as it would be encountered in the operating room (OR), hence, being useful for planning a patient-tailored procedure. This could possibly help inexperienced surgeons before going into an OR as well as senior surgeons who are approaching challenging procedures.
Uterine fibromatosis is common in women, with an estimated prevalence of up to 15%–50% after age 35. About 80% of women affected by fibromatosis have symptoms (including bleeding, menstrual and pelvic pain, and infertility) and require treatment, including surgical ablation. Surgical procedures for patients with myomas include hysterectomy or myomectomy.4,5 Both procedures can be challenging for multiple reasons. Bulky myomas offer relevant challenges, even to experienced surgeons, and often limit the possibility to achieve hysterectomy in a minimally invasive fashion. 6 Myomectomy can be even more challenging, because extensive ablation of myomas needs to be achieved while preserving the function of the uterus. Location, number, and accessibility of myomas all represent technical difficulties. 7 Currently, gynecologists use ultrasound to map uterine leiomyomas during preoperative work-ups. In expert hands, 2D ultrasonography identifies the number and the localization of leiomyomas with high sensitivity and specificity. 8 However, computer-assisted anatomical reconstruction of the uterus and of myomas would be useful as a support for preoperative planning (i.e., hysterectomy versus myomectomy, open versus mini-invasive approach) and possibly for the surgery itself (e.g., potential for more-rapid identification of myomas, reduced surgical time and bleeding).
Volumetric images acquired with MRI or other techniques potentially contain the 3D information that could help a surgeon. For efficient visualization of that kind of information, direct volume rendering algorithms are not useful. Dataset segmentation is required to obtain a clear surface rendering of the required anatomy.9–11 The segmentation process consists of dividing images into constituent subregions. Segmentation tools can be divided into three groups according to the level of automaticity: (1) automatic; (2) semiautomatic; and (3) manual. Manual segmentation is totally made by an operator, representing a time-consuming task with potential operator variability, while automatic and semiautomatic segmentations are realized with total or partial computer elaboration with an operator validating the results to correct possible errors.9–14
The current authors performed a prospective study on 18 premenopausal women scheduled for surgical treatment for uterine fibromatosis who underwent pelvic MRI for unrelated reasons. All of the patients had already been evaluated by a single surgeon and assigned specific surgical plans based on US and gynecologic examinations (open versus laparoscopic surgery, hysterectomy versus myomectomy). For these patients, 3D reconstructions were obtained, using semiautomatic segmentation and computer-assisted image elaboration, and the images were shown to the surgeon before the final scheduling of each procedure.
The study analysis comprised the changes in surgical planning toward a less-invasive or to a more-conservative technique (e.g., from an open procedure to a laparoscopic approach; from hysterectomy to myomectomy) selected by the surgeon upon being exposed to a re-evaluation of the patient with the 3D images. Successful completion of the modified surgical plan was one of the outcomes. The 3D reconstructions were shown to the surgeon during the procedure and the numbers of visualizations of the images were assessed as well as their effects on rapidity and efficacy of removal of the myomas. In all cases, anatomical reconstructions of the locations of the myomas were obtained at the time of surgery. Specificity and sensitivity to locate the myomas correctly was tested for the 3D reconstruction technique, compared to the preoperative US scan. Finally, surgical data were analyzed from 30 consecutive patients with comparable characteristics who were scheduled for fibromatosis surgery in the same period of time. No 3D reconstruction was available for these patients. This allowed comparative assessment of the mean time to locate and remove each myoma based on the pre- and intraoperative availability of the 3D reconstruction of these myomas.
Materials and Methods
Patients' characteristics
Between October 2015 and June 2016, 18 consecutive patients with uterine fibromatosis selected for surgery and assigned to one single surgeon (T.S.) were prospectively enrolled in the study in the Division of Obstetrics and Gynecology of the University of Pisa. Patients had to undergo pelvic MRI in order to investigate their different concomitant gynecologic pathologies (ovarian cysts, chronic pelvic pain, etc.). All patients had symptomatic leiomyomas (dysmenorrhea, bleeding, pelvic pain, infertility). A parallel group of 30 consecutive patients presenting to this institute during this time period with clinical and anatomical conditions similar to those of the previously described patients and scheduled for surgery due to symptomatic uterine fibromatosis was also enrolled in the study. These 30 patients did not undergo pelvic MRI due to lack of indications. Informed written consent was obtained from all patients.
MRI image acquisition protocol and 3D reconstruction
MRI was performed with a 3T system (GE 750 Discovery; General Electric) using an 8-channel phased-array coil. The MRI protocol included a 3D fast T2 weighted sequence (CUBE) with the following technical parameters: TR/TE 1500–1900/102–107, matrix 224–320 × 256–320, echo train length 80–90, slab partitions' thickness 2.2 mm ZIP 2, FOV 28 × 25.2, bandwidth 62.5 Hz, and acquisition time ∼5–6 minutes. CUBE allows obtaining an isotropic 3D images dataset useful for a reconstruction with high spatial resolution and high contrast. No contrast medium was used for imaging and the total duration of the examination was ∼20 minutes. In every case, MRI images were segmented after being made anonymous and stored in separated directories organized by patient number and phase identifier. Patient-specific 3D models were generated using a semiautomatic tool 12 that was integrated into the open-source software ITK-SNAP 1.5 13 * (Fig. 1).

The processing of endometrial cavity
The whole segmentation procedure is based on the neighborhood-connected region growing algorithm appropriately parameterized for the specific anatomy.
The basic algorithm integrated in the “EndoCAS segmentation pipeline” was guided by the radiologist in the process of generating 3D image reconstruction. During segmentation, the topology of segmented structures was validated by the radiologist and corrected if necessary. The system allowed generation of 3D uterine models in ∼30 minutes. Manual refining through a touch screen monitor was available for structures that were not picked by automatic/semiautomatic segmentation. This software provided different types of manual segmentation tools, such as a pen to plot points (with different sizes and shapes and with the possibility of plotting 3D points) or contours (automatically filled). Manual refinement and segmentation was frequently required for MRI images of uterine fibromatosis.
The segmentation was performed by radiologists with the support of surgeons and engineers. The lead surgeon (T.S.) was never involved in the segmentation process. Each anatomical structure was highlighted with a different color. At the end of this technical process, a patient-specific 3D model of the anatomy relevant to each of the 18 procedures was obtained.
From a technical standpoint, reconstruction of the uterus and myomas consisted of a series of steps. The first segmentation step involved the endometrial cavity (Fig. 1). This was an easy structure to obtain an image of with semiautomatic segmentation, given the cavity's high signal intensity. Afterword, manual segmentaion of myomas was performed, using a software tool for the insertion of spheres in the 3D model. The operator scrolled the MRI slices to find the center of each myoma. Then the diameter of the sphere was modulated to match, as precisely as possible, the myoma borders (Fig. 1). The approximation of the shape of the myomas to a spheric geometry fitted most myomas fairly enough, and was able to reproduce successfully the anatomical shape of the uterus that was required to simulate this kind of surgery. Processing the uterus was the last step (Fig. 1). This was a totally manual phase, given that no segmentation algorithm able to work with this kind of images was found. Slice by slice, the current author proceeded to identify the uterus contour and the program automatically filled the surface with a selected color. This step was made easier by the use of a touch screen.
Description of the study
Patient-specific 3D models of uteri were provided to the surgeon (T.S.) 2 days before surgery, at the time of the final rehearsal with the patient to confirm the preselected surgical program. The surgeon was able to visualize the 3D models from different points of view and to rotate the model in order to obtain complete information about each patient's specific anatomy (Fig. 2). At this timepoint, modifications in the original surgical plan—based on repeat gynecologic examinations, and transvaginal US (TVUS) and transabdominal US scans—integrated by the anatomical information provided by the 3D models were recorded. Specifically, changes from a laparotomic approach toward a laparoscopic technique and changes from a hysterectomy to a myomectomy plan were evaluated. A similar reevaluation visit was also parformed for the 30 consecutive comparator women scheduled for surgery during the recruitment period. In these, women a new gynecologic examination and TVUS and transabdominal US scans were performed. No changes were made in the originally planned surgical programs in any of the cases for whom the 3D models were not available. All patients were preevaluated and reevaluated, and later operated by the same surgeon (T.S.).
Visualization of the three-dimensional models from different points of view and rotation of the model in order to achieve complete information about the patient-specific anatomy.
During surgery, patient-specific 3D models were made available to the surgeon. An analysis of the number of views and the relationthip with the complexity of the surgery was performed.
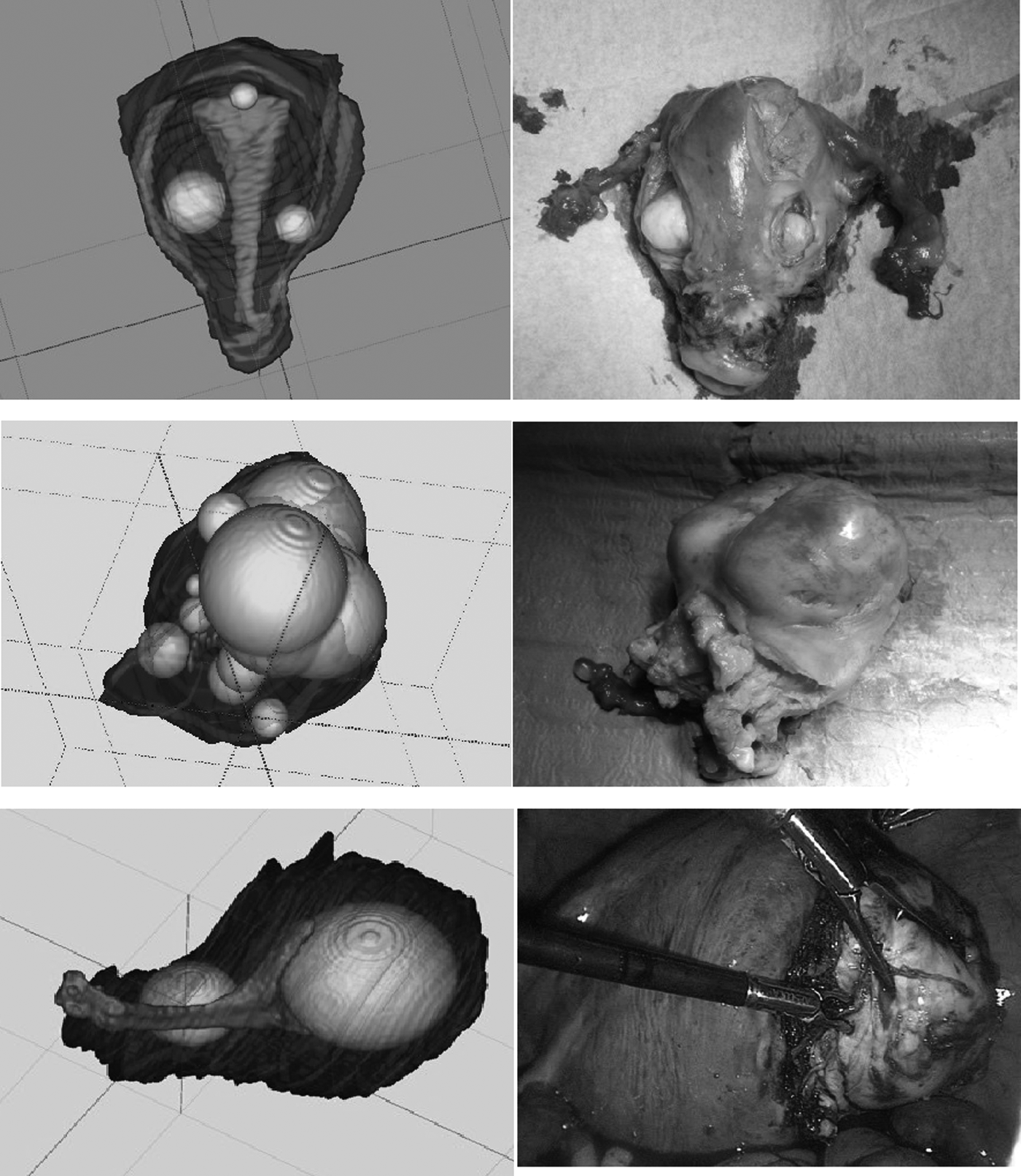
During surgery, a thorough assessment of the numbers and exact locations of the myomas was performed. This allowed comparing the MRI-based 3D reconstructions with the US scans in terms of sensitivity (or the ability to identify the presence of all myomas correctly) and specificity (or the ability to correctly identify the anatomical position of all myomas; Fig. 3).
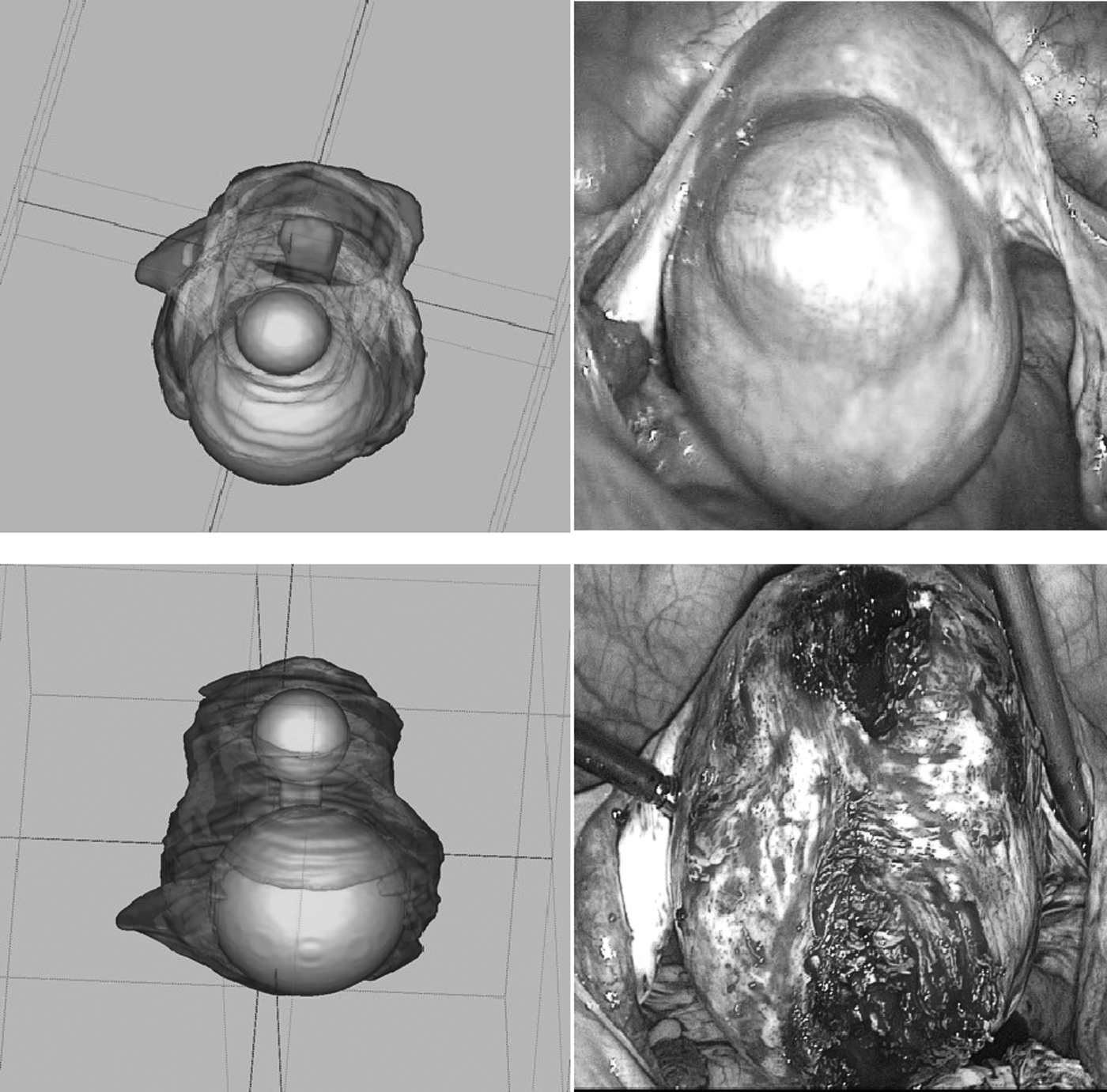
Assessment of the number and exact location of the myomas performed during surgery. This allowed comparison of magnetic resonance imaging–based three-dimensional reconstruction with the ultrasound scan.
Other recorded outcomes of the study were the ability to complete the scheduled surgical plans successfully, along with intraoperative and post-operative hematocrit and hemoglobin drops, hospital stays, and any complications.
Finally, the time needed to surgically identifiy and extract the myomas (when myomectomies were performed) was recorded in all patients for whom MRI-based 3D models were available and compared to the cases for whom these reconstructions were not available.
Preoperative evaluations included medical history, physical examinations, and laboratory tests for all patients. All patients were counseled about the risks, benefits, and alternative treatments, and signed informed consent forms. Institutional review board approval was obtained by the ethical committee of the University of Pisa.
Design of the study and statistical analysis
This was a prospective, nonrandomized study. Data analysis was performed with software: SPSS version 1.4. Descriptive statistical analysis (means, standard deviations [SDs], and percentages) was performed using Student's t-test. Significance was set at p < 0.05. Statistical comparison of the sensitivity of US versus MRI plus reconstruction techniques between the 2 groups was performed using χ2 and Fisher's exact test.
Results
Impact of the MRI-based patient-specific 3D reconstruction of the uterus on surgical planning
When the patient-specific 3D images depicting the anatomy of the fibromatosis were shown to the surgeon at the final rehearsal when the surgical plan is definitely scheduled, changes in the surgical plans were decided in a significant number of the patients. Specifically, of the 18 patients enrolled in the MRI group, 6 were originally scheduled to undergo open procedures. Upon visualization of the 3D reconstruction, 4 of these patients (66.6%) were shifted to minimally invasive laparoscopic surgery. Moreover, 5 of 12 patients (41.6%) for whom laparoscopic hysterectomy had been planned were chosen for conservative myomectomy upon visualization of the images.
Sensitivity of TVUS versus MRI plus reconstruction techniques
Sensitivity of the MRI-based 3D imaging system was higher than TVUS. Specifically, 97% of myomas were detected with the 3D reconstruction versus 72% with TVUS (p = 0.125). The intrauterine position of 98% of the myomas was identified correctly when using the MRI-based 3D reconstruction system. In parallel, TVUS allowed correct identification of the position of 76% of the myomas (p = 0.228). Both differences were not considered to be statistically significant, probably, because of the small number of enrolled patients, despite the evident and different trends.
Time needed for surgical removal of the myomas
An assessment was made regarding whether or not pre- and intrasurgical availability of the 3D reconstruction images helped the surgeon to complete the procedures more quickly. To this extent, the current authors evaluated the time spent to identify each myoma during laparoscopic conservative myomectomies when 3D reconstruction of the anatomy was available (n = 9). Specifically, the time needed from uterine incision to complete removal of each myoma was measured (excluding the time needed for suturing). As a comparator, the same parameters were measured in a set of 30 patients with similar clinical features, and who were undergoing laparoscopic myomectomy. In patients with 1 or 2 leiomyomas, the average time needed to identify and remove each myoma was 7.3 ± 1 minute if the 3D images were available, compared with 12.2 ± 1 minute in controls (p < 0.0001).
On the contrary, patients enrolled for myomectomies with more than 2 leiomyomas and who previously underwent MRI and reconstruction, the average time for removal was 37.8 ± 4 minutes, compared with 23.1 ± 5 minutes in control patients (p < 0.0001).
Surgical outcomes
Other parameters that were also looked at included possible changes in total surgical times, hematocrit and hemoglobin drops, hospital stays, and postoperative fevers, in the 2 analyzed groups of patients. No statistically significant differences between patients who previously underwent MRI with 3D-reconstruction and patients who underwent TVUS were found in total surgical time, hematocrit and hemoglobin drops, hospital stays, and postoperative fevers.
Intraoperative consultation of images
The analysis of surgeon intraoperative consultation of images showed significant differences between complex and simple fibromatosis. Therefore, during surgery for myomectomy of more than 2 leiomyomas, the surgeon consulted images about four times (mean ± SD: 3.83 ± 0.7) in comparison with 1.25 ± 0.6 times during myomectomy of 1 or 2 leiomyomas (p < 0.0001).
Discussion
The main result of this study was demonstration of the relevance of an MRI-based imaging system with 3D-reconstruction of the uterus and the pelvis in pre- and intraoperative phases in gynecologic surgery for uterine fibromatosis.
The observation of 3D volumetric imaging seems to be a true improvement in gynecologic reproductive surgery; indeed the creation of virtual reality 3D models of uteri, sizes and locations of myomas contributes to tailored procedures addressing each individual anatomical patient characteristics. In the current authors' opinion, tailoring anatomical models resulted in changes of surgical planning, increasing minimally invasive techniques and favoring conservative approaches to uteri even in the most complicated conditions; thus preserving reproductive function.
The results showed that 22.2% of patients with fibromatosis enrolled for open abdominal approach underwent minimally invasive surgery. Moreover, in 31.2% of patients selected for total laparoscopic hysterectomy, surgical planning was modified to conservative myomectomy. Probably, higher sensitivity of MRI and 3D reconstructions, compared with TVUS, gives additional information to surgeons. In the OR, patient-specific 3D visual-models obtained after segmentation allows surgeons to proceed with knowledge of precise number and localization of leiomyomas, and provides more-intuitive ideas of anatomical landmarks. For simple fibromatosis (1–2 myomas), time required to search for each lesion can be reduced and a surgeon can approach critical interventions with a major awareness of each patient's specific anatomy.
On the contrary, in women with more than 2 leiomyomas, time for removal of each lesion was longer in patients with previous MRI and 3D reconstruction, but it is plausible that segmentation allowed better understanding concerning the anatomical relationships of the target structures. This, in turn, induced a change in the surgical strategy in some cases, letting some patients originally selected for a demolitive approach preserve their uteri.
As demonstrated in these results, sensitivity and specificity of MRI and 3D reconstruction are widely higher than US; indeed, it is well-known that, when there were increased numbers and sizes of leiomyomas—especially in massive fibromatosis—US progressively showed lower accuracy, often giving inadequate or wrong information. 8
Although US anatomical information sometimes seems to be similar to MRI-generated information, the main role of MRI and 3D reconstruction is crucial for generating an intuitive topographic map of the uterus, so that a surgeon can organize the information and build a mental-operative scheme in presurgical planning as well in the intraoperative phase.9,10
This concept is crucial and well-elucidated by the analysis of surgeon intraoperative consultation of images, which showed significant differences between complex and simple fibromatosis; indeed, during surgery for myomectomy of more than 2 leiomyomas, the surgeon consulted reconstructed-3D images about four times more, in comparison with once during myomectomy for 1 or 2 leiomyomas.
An accurate correspondence between reconstructed 3D virtual images and real anatomy was found, while US was not able to provide analogous results.
Nevertheless, according to the analysis of surgical times, hematocrit and hemoglobin drops, hospital stays, and postoperative fevers, we found no statistically significant difference between patients who previously underwent MRI with 3D reconstruction and patients who underwent only US in different analyzed groups. This could be likely because, in patients with massive fibromatosis selected for total hysterectomy, MRI and 3D reconstruction did not change pre- and intraoperative planning and the complexity of clinical conditions indicated a plan of demolitive surgery.
Similarly, as previously explained, in patients selected for multiple complex myomectomies, MRI and 3D reconstruction did not produce any statistically significant difference in perioperative outcomes, but the intraoperative identifications of detailed anatomical landmarks could have allowed a conservative or minimally invasive approach. A limitation of the current study is the small number of both patients in the MRI and control groups.
Conclusions
Although generation of 3D models segmenting images still remains a complex procedure that is considerably time-consuming—thus not feasible in quotidian medical practice—the models are useful in complex cases associated with preoperative ultrasound examinations. The relevance of these models, as evidenced by this small prospective study, is well-recognized by the final user—the operating surgeon.9–12 However, use of the models can also be supported by nonmedical staff according to the results for cases in which MRI and 3D reconstruction allowed the choice of a better surgical strategy. Therefore, in the current authors' opinion, the development of automatic software associated with US examination could be likely and suitable.
Consequent, prospective pre- and intraoperative application of this imaging technique demonstrated that it was feasible and surgically relevant, and provided substantial support for gynecologic surgery to achieve the essential goals of modern reproductive surgery.
Further studies are necessary to quantify clinical improvements of MRI and 3D reconstruction for complex uterine fibromatosis.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest.