
Abstract
Abstract
Background:
Bilateral mature cystic teratomas are seen in only 10% of cases. Furthermore, the occurrence of endometrial cancer in this setting is extremely rare.
Case:
A 62-year-old woman presented with postmenopausal bleeding. On transvaginal ultrasound, bilateral complex ovarian masses, that raised suspicion of dermoid cysts with hypoechoic endometrial collection, were detected. Endometrial sampling showed inflammatory changes, and her Papanicolaou smear was normal. Her CA-125 was normal. During exploratory laparotomy, bilateral dermoid cysts of 7 × 7 cm were detected along with thickened endometrium.
Results:
Final histopathologic diagnosis confirmed benign mature cystic teratomas coexisting with moderately differentiated endometrial cancer, with less than half thickness of myometrial invasion.
Conclusions:
Bilateral mature cystic teratomas and endometrial cancer is an incidental finding. In all cases of postmenopausal bleeding with bilateral dermoid cysts, a strong suspicion of endometrial cancer must be kept in mind. The combination of these two conditions is unique, and, to the best of the current authors' knowledge, has not been reported previously in the English-language medical literature. (J GYNECOL SURG 2017:1)
Introduction
A
Case
A 62-year-old woman, para 3, live 3, presented to a gynecologic outpatient department with complaint of postmenopausal bleeding of 1½ months' duration. She had attained menopause 13 years prior. Her family and personal history were negative for gynecologic, breast, and colorectal cancers. On examination, her body mass index was 27 kg/m2. Per abdomen and per speculum examinations were unremarkable. A bimanual examination revealed masses in both fornices of ∼6–7 cm and 7–8 cm in the right and left sides, respectively. Laboratory findings were: CA-125, 21.40 IU/mL; preoperative hemoglobin,10g/dL; blood urea, 30; and serum creatinine, 0.8 mg/dL. On transvaginal ultrasound, both ovaries appeared to be bulky. There were large, unilocular cystic lesions that had internal echoes with hyperechoic contents. The cysts measured 7.1 × 5.8 cm on the right side and 5.8 × 6.8 cm on the left side, which was suspicious of dermoid cysts, with mild hypoechoic collection in the endometrial cavity. Her uterus was normal. Her Papanicolaou smear was normal, and endometrial sampling showed inflammatory changes.
She underwent an exploratory laparotomy through a lower midline vertical incision. During the laparotomy, 7 × 7–cm bilateral ovarian tumors with smooth capsules and cystic consistency were detected, while her uterus and bilateral fallopian tubes were normal (Fig. 1). Peritoneal washings were collected. Clockwise intra-abdominal palpation did not reveal any abnormalities. Peritoneal and omental biopsies were taken. A total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed. On cut section of both ovarian masses, sebaceous material emerged and teeth were identified. Her uterus contained thickened endometrium.

Intraoperative view of bilateral dermoid cysts of the ovaries with smooth capsules and a normal-appearing uterus.
Results
This patient was discharged on the tenth postoperative day, with her postoperative period being uneventful. A histopathologic report confirmed the diagnosis of moderately differentiated endometrial cancer invading less than half of the myometrium (Fig. 2), with the uterocervical junction being free from infiltration. Her cervix showed chronic cervicitis, her ovaries had bilateral mature cystic teratomas (Fig. 3), while the peritoneum and omentum were free from tumor infiltration. Peritoneal washings were negative for malignant cells.
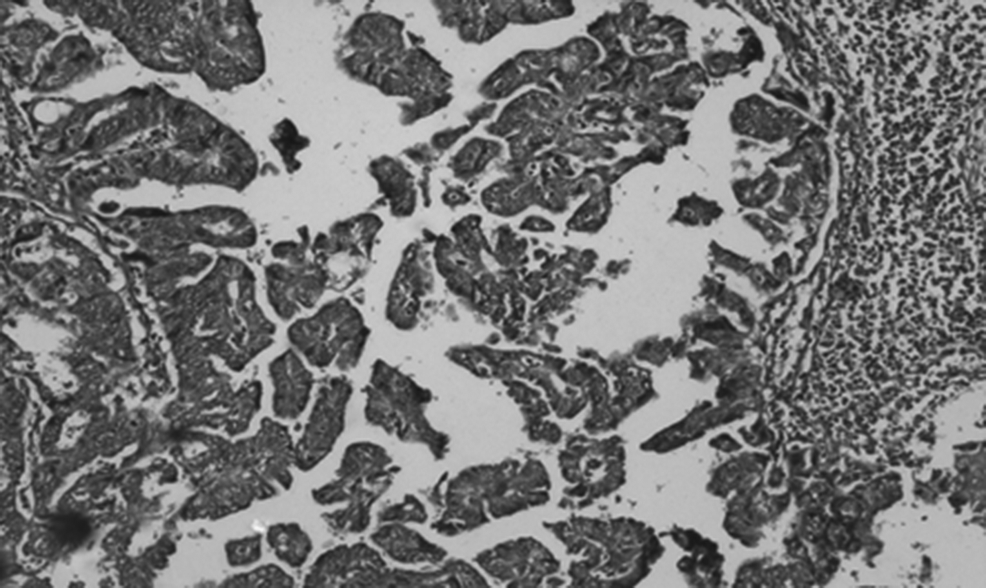
A 10 × 2 microscopic picture of moderately differentiated endometrial cancer with less than half thickness of invasion in the myometrium (H&E).
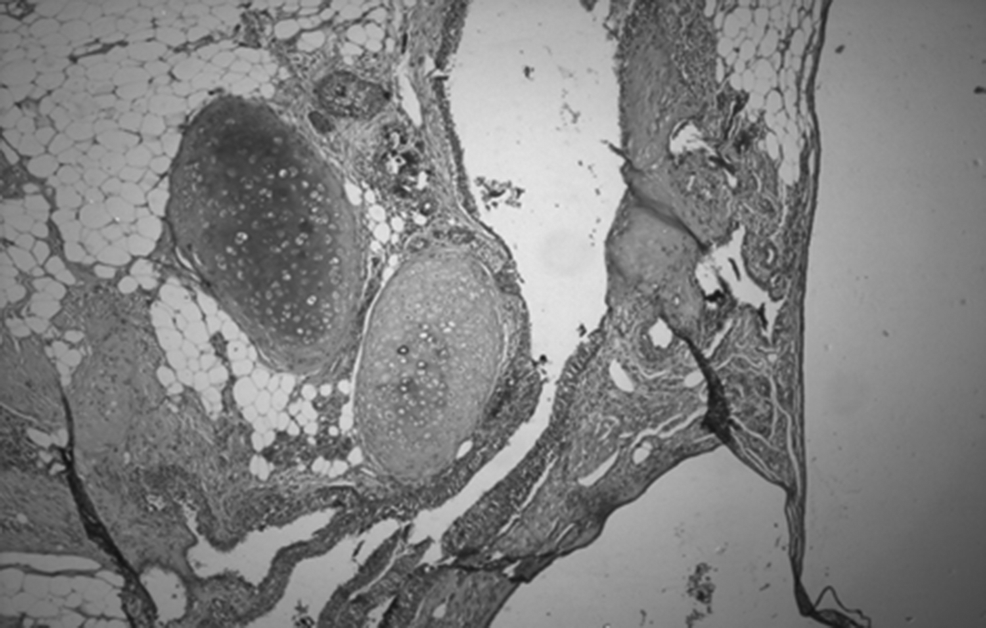
A 4 × 2 microscopic picture showing a mature cystic teratoma of the ovary (H&E).
Discussion
Teratomas can be mature or immature. Both mature and immature types of teratomas are benign, but an immature teratoma has a more-aggressive course. 2 The disease occurs in patients of almost any age, from childhood to postmenopause, although the peak incidence is reported in women age 20–40. 3 Mature cystic teratomas are usually slow-growing, with an estimated growth rate of 1.8 mm/year, 4 and have arrested growth after menopause. Bilaterality is usually seen in 10%–15% of cases. In adults, dermoid cysts are asymptomatic in 64.5% of cases 5 and are commonly incidental findings during imaging or surgical procedures for other reasons, whereas, in children and adolescents, these cysts usually present with abdominal pain and distension.
Torsion is the most common complication, whereas rupture and suppuration are uncommon, due to the tumors' thick capsules. 5 Malignant changes are uncommon and occur in 0.1%–0.2% of cases. 6 Squamous-cell carcinoma (SCC) is the most common malignant change. Predictors of malignant change are elevated CA-125 levels, older age, large tumor masses, and postmenopausal status. 7
Some of the associations found in the literature on bilateral dermoid cysts are hemolytic anemia, 8 endometriosis, and ectopic pregnancy. 9 There is only one report so far regarding SCC arising from a mature cystic teratoma of the ovary with synchronous endometrial adenocarcinoma. 10 Although the dermoid cysts in the current case had risk factors for malignant transformation—such as older age, postmenopausal status, and large size—there was no focus of SCC arising from the cysts. Instead, there was coexisting endometrial cancer. Thus, there can be a possibility that dermoid cysts have the potential to stimulate residual ovarian stroma for estrogen production and, consequently, lead to endometrial cancer. Further studies are needed to confirm this speculation. However, the combination of bilateral mature cystic teratomas and endometrial cancer is unique and, to the best of the current authors' knowledge, this has not been previously reported in the English-language medical literature.
Conclusions
Bilateral mature cystic teratomas and endometrial cancer are incidental findings. In all cases of postmenopausal bleeding with bilateral dermoid cysts, a strong suspicion of endometrial cancer must be kept in mind. Magnetic resonance imagine could have probably helped to make a preoperative diagnosis of endometrial cancer and myometrial invasion, and to determine the exact characterization of the ovarian masses.
Footnotes
Acknowledgments
The authors are thankful to Sunita Singh, MBBS, MD, a professor in the department of pathology, of the Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, Rohtak, in Rohtak, India, who provided the histopathology slides for this article.
Author Disclosure Statement
The authors of this article have no conflicts of interest with respect to publication of this article.