
Abstract
Abstract
Background:
Malignant melanoma of the uterus is a very rare disease entity bearing potentially serious consequences with an unpredictable and poor prognosis.
Case:
A 64-year-old woman who had a longstanding, slow-growing blackish mass of the right big toe for more than a decade, presented with postmenopausal bleeding. Histopathologic examination confirmed the diagnosis of a likely secondary malignant melanoma of the uterus.
Results:
She was treated successfully without any complications via total laparoscopic hysterectomy and bilateral salpingo-oophorectomy (TLHBSO). Even though malignant melanoma of the uterus has a poor prognosis, the patient was alive and disease-free at a 1-year regular follow-up.
Conclusions:
A malignant melanoma of the uterus is very rare and has a poor prognosis. However, laparoscopic excision of the uterus and adjacent organs in selected patients could be a superior option, especially in terms of rapid recovery and minimal tumor spillage. A combined multidisciplinary approach is highly recommended for dealing with malignant melanoma–related diseases for optimal care and a better clinical outcome. (J GYNECOL SURG 33:149)
Introduction
M
The prognosis of a malignant melanoma of the uterus has been reported to be poor despite radical hysterectomy, bilateral salpingo-oophorectomy, and pelvic-node dissection. There is no absolute optimal treatment in malignant melanoma of the uterus due to its rarity and unpredictable prognosis. 5
This article presents a rare case of a metastatic malignant melanoma of the uterus in a patient who presented with postmenopausal bleeding and was treated successfully via laparoscopic surgery. This is an exceptionally different mode of definitive treatment for tumors confined to the uterus, compared to conventional open surgery. To the current authors' knowledge, this is the first reported case of a malignant melanoma of the uterus in Malaysia.
Case
A 64-year-old Chinese woman, para 4, who was 14 years postmenopausal and not receiving hormonal replacement therapy, presented with a 2-month history of abnormal vaginal bleeding. There were no constitutional symptoms and no family history of malignancy. She was apparently well with no known medical illness with the exception of an abnormal growth on her right big toe that had been there for more than a decade. It was a slow-growing, painless, and non-foul–smelling blackish growth, which had grown from a pea size until it gradually involved almost the whole of the toe and some part of the second toe (Fig. 1). This growth had been untreated until this patient presented with her postmenopausal bleeding.

Cutaneous melanoma involving big toe and some part of the second toe of right foot.
Upon admission of this patient, a pelvic examination revealed a bulky uterus with no lesions noted at the vulvo–vagina and cervix. The parametrium was free. Ultrasound showed an 8 × 4–cm uterus and a 3 × 4-cm submucosal uterine fibroid with a 7.7-mm endometrial thickness. The patient underwent hysteroscopy and endometrial curettage plus a biopsy of the right big toe. Both samples revealed malignant melanoma. A computed tomography scan of the thorax, abdomen, and pelvis showed no evidence of extracorporeal lesions.
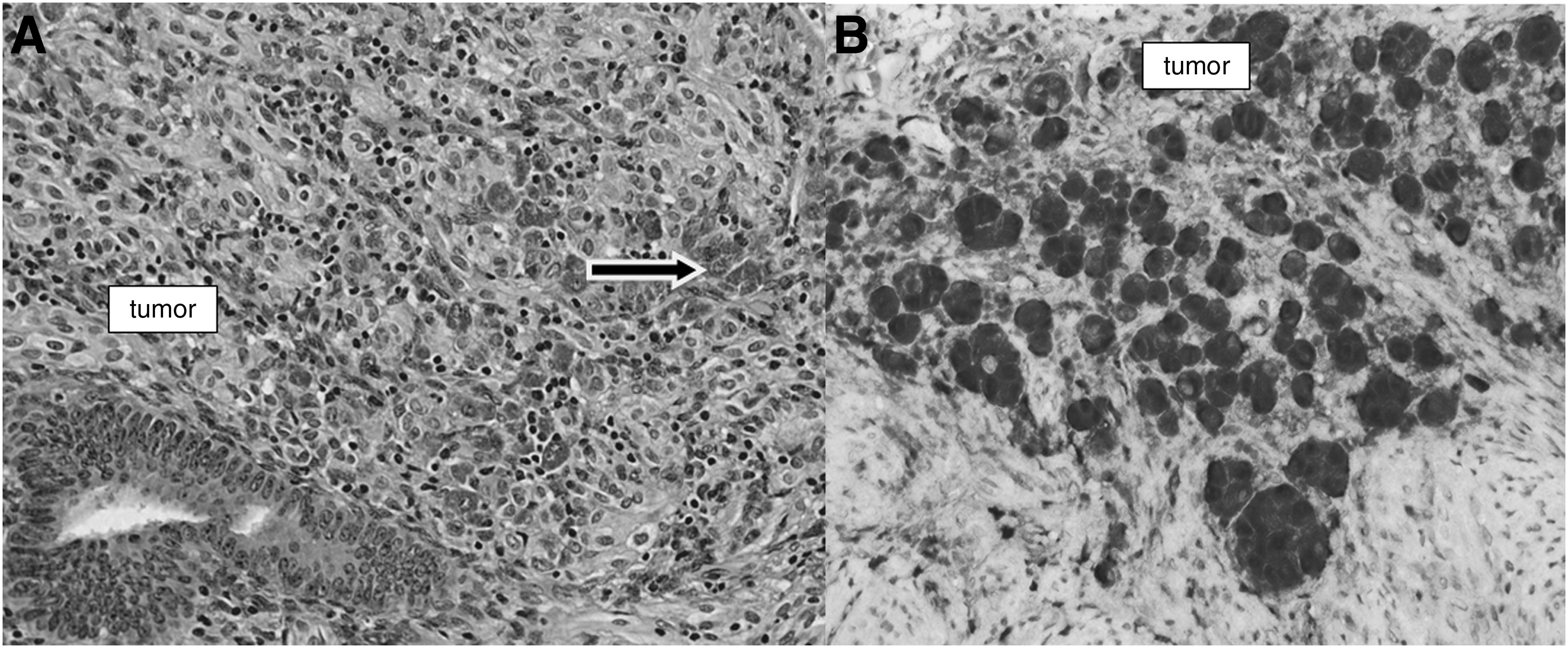
The patient was managed via a multidisciplinary approach involving a gynecologist, dermatologist, orthopedic surgeon, and oncologist. The patient underwent a right big toe and second toe amputation, followed by a total laparoscopic hysterectomy with a bilateral salpingo-oophorectomy (TLHBSO) at a 6-week interval. Macroscopic examination of the specimens showed multiple blackish ill-defined tumor lesions involving the endomyometrium and endocervix, ranging from 2 mm to 28 mm. The ectocervix, both ovaries, and fallopian tubes were free of tumors (Fig. 2). Histopathologic examination confirmed the presence of a uterine malignant melanoma. This tumor showed positive immunoreactions to HMB45, Melan A, Vimentin, and S 100. The melanocytic pigments were highlighted by a Masson Fontana stain. The tumor showed a negative immunoreaction to cytokeratin markers (Fig. 3).
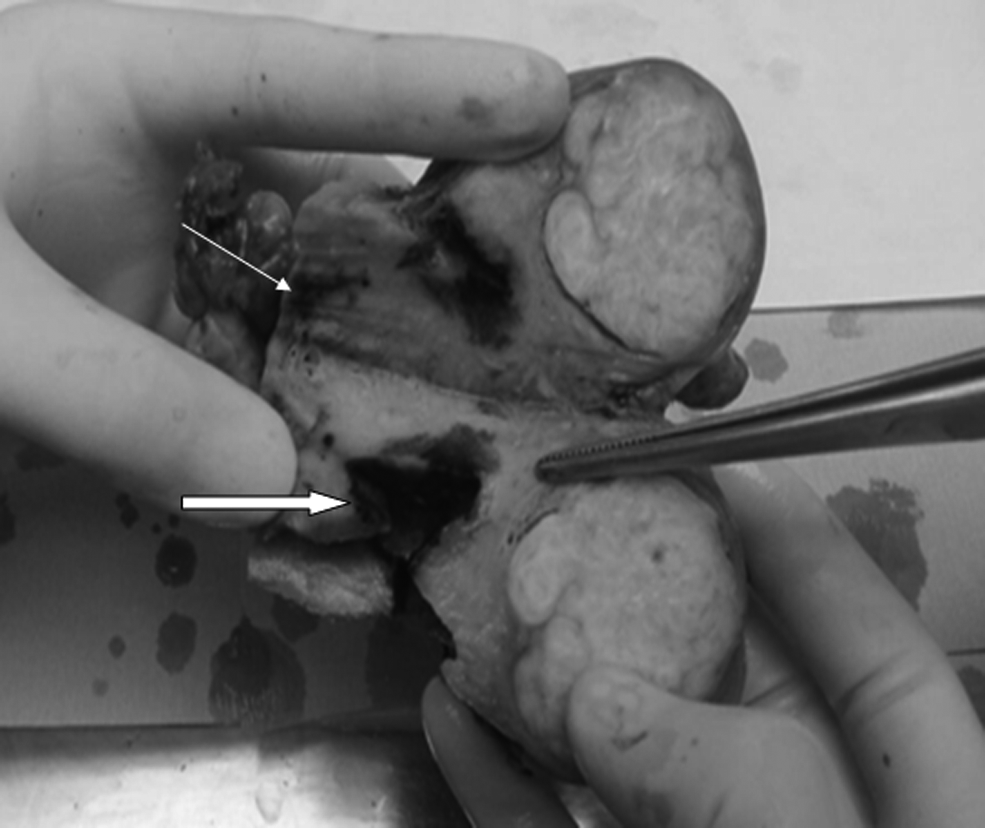
Macroscopic findings reveal a blackish tumor involving the endometrium and extending into the myometrium (thick arrow). Tumor deposits are also noted at the endocervical region (thin arrow).
Results
No adjuvant therapy was instituted, as the tumor had been resected with clear margins. The patient had an uncomplicated postoperative recovery. At 1 year postoperation, she was alive and disease-free. She was able to resume her daily activities and had no active symptoms that required further medical attention.
Discussion
A malignant melanoma is a highly malignant tumor that is predominantly >95% cutaneous in origin. Of all noncutaneous malignant melanomas, only 1% involve the mucosal layers in the oral–nasal cavity, gastrointestinal (GI) tract, and genital tract. 6 Most malignant melanomas in the genital tract predominantly involve the vulva and vagina and, in some studies, there is a documented incidence of malignant melanomas of the genital tract as low as 0.03%–0.5%.2,4,7 Malignant melanoma of the uterus is an extremely rare neoplasm of which only <100 cases have been reported. 4 Only 11 cases are documented in the literature as malignant melanomas that were metastatic specifically to the endometrium. 8
The occurrence of a melanoma of the uterus can be either a primary or a metastatic tumor. The most common extragenital metastatic melanomas of the uterus are from the breast and GI tract. 9 However, extragenital metastatic melanomas have also been reported with primaries from a number of other sites, such as the skin, uvea, or hard palate.3,10
The majority of cutaneous malignant melanomas occur in women with white skin or other fair complexions. 4 In Asia, Chinese ethnicity has been predominantly involved as described in a study undertaken in Singapore. 11 However, there has been no such study to investigate the prevalence of noncutaneous melanomas, especially in the uteri in patients of different ethnicities.
The incidence of malignant melanomas of the uterus is more common in older age groups of women and is predominant among postmenopausal women, compared to younger-age groups. 5 The usual clinical manifestation is abnormal uterine bleeding, as seen in the current case, which prompted the patient to seek medical attention. In this particular case, the tumor appears to have been confined to the right big toe and, in addition, there was no evidence of extensive tumor spread at the time of diagnosis, which altogether conferred a better prognosis for this patient.
Given that malignant melanoma is the greatest mimicker among all tumors, a high-index of suspicion, careful morphologic assessment and immunohistochemical studies are necessary when developing the final diagnosis. A thorough clinical assessment will always aid in the diagnostic workup. The production of melanin pigments may provide a clue; in cases with subtle pigment production, immunohistochemical tests—such as S-100 protein, anti-Mart-1/Melan-A, and HMB-45—need to be performed in order to arrive at the right diagnosis. In this patient, the tumor cells were positive for S-100, Melan-A, HMB-45, and Vimentin. A special histochemical stain, Masson Fontana, can also be utilized to confirm the presence of the melanin pigment.5,8
There is currently no absolute or optimal treatment protocol for the management of malignant melanoma of the uterus due to the rarity and unpredictable prognosis of this melanoma. However, radical hysterectomy with bilateral salpingo-oophorectomy and pelvic-node dissection without chemo/radiation therapy has been recommended as treatment.1,5,7,8 In the current case, the primary site (the right big toe) and the metastatic site (the uterus) were successfully removed through surgical intervention. Given that there was no evidence of further organ involvement by the tumor, it was presumed that the tumor was localized in the female genital tract only. Thus, TLHBSO were performed as definitive treatment. In all the case reviews, no surgical intervention was performed laparoscopically, unlike in the current patient in whom TLHBSO was performed with a good postoperative outcome. This shows that, in selected patients, there is a role for laparoscopic surgical intervention by a trained surgeon.
It has been stated that melanoma of the uterus, whether primary or secondary, has a poor prognosis.3–5,12 Additional chemo/radiation treatment is only suggested in a particularly advanced stage of the disease. Currently, a chemotherapy protocol using dacarbazine alone is as effective as any combination therapy used. 8 A malignant melanoma is a radio-resistant tumor. Therefore, radiotherapy is not a primary treatment for a malignant melanoma and is only an option for advanced disease, recurrent disease, an unsatisfactory surgical margin, residual tumors, and pelvic lymph-node involvement. 7 Other new adjuvant treatments have been suggested, such as immunotherapy and interferon-α. However, the effectiveness of these treatments remains statistically unproven and experimental. Ideally a multicenter trial or systematic review regarding the treatments given needs to carried out in order to both ascertain the best treatment option and improve the prognosis of patients.
Conclusions
A malignant melanoma of the uterus is very rare and has a poor prognosis. However, the current authors believe that laparoscopic excision of the uterus and adjacent organs in selected patients could be a superior option, especially in terms of rapid recovery and minimal tumor spillage. A combined multidisciplinary approach is highly recommended in dealing with malignant melanoma related diseases for optimal care and a better clinical outcome.
Footnotes
Acknowledgments
The study's authors are grateful to all the medical officers and staffs for supporting and assisting us. We would also like to thank the director general of Health Malaysia for his permission to publish this article.
Author Disclosure Statement
There are no potential conflicts of interest to report, financial or otherwise.