
Abstract
Abstract
Background:
Emergent peripartum hysterectomy is warranted for a variety of indications, including uterine rupture, uterine atony, retained placenta, and abnormal placentation. Abnormal placentation is an increasingly common phenomenon that can be attributed to disruptions in the endometrial decidua following cesarean delivery, myomectomy, dilation and curettage, endometritis, endometrial ablation, and other operative procedures.
Case:
At 10 weeks of gestation, a patient with two previous cesarean deliveries and two terminations of pregnancy via dilation and curettage underwent a suction dilation and curettage for a missed abortion. Hemorrhage occurred; she became hemodynamically unstable and underwent an emergent total abdominal hysterectomy (TAH).
Results:
Surgical pathology testing confirmed an intracervical pregnancy with a placenta accreta.
Conclusions:
This case highlights the difficulty in differentiating cervical ectopic pregnancy with a spontaneous abortion in process. In order to prevent loss of reproductive function, massive hemorrhage, and possibly maternal mortality, the current authors recommend that, in patients with histories of multiple cervical instrumentations, the risk of cervical ectopic pregnancy and even abnormal cervical placentation must be considered in the preoperative differential. In the unstable patient, the “gold standard” treatment for abnormal placentation—TAH—is warranted when conservative measures, such as balloon tamponade, fail. (J GYNECOL SURG 33:215)
Introduction
E
Case
A 32-year-old woman, gravida 5, para 2022, presented at 5 weeks and 5 days of gestation, with an estimated date of confinement of February 17, 2017, based on her last menstrual period May 13, 2016. She had an obstetrical history that was significant for two full-term lower transverse cesarean deliveries and two terminations of pregnancy via dilation and curettage, with no medical problems and no additional surgical history. She underwent a routine dating and viability ultrasound (US). The US showed a gestational sac measuring 4.0 cm—corresponding to a gestational age of 10 weeks and 1 day—located in the lower portion of her uterus, without an identifiable yolk sac or fetal structures. The diagnosis was an abnormal gestational sac in the lower uterine segment, raising suspicion of an abortion in progress (Fig. 1). The patient elected evacuation via suction dilation and curettage.
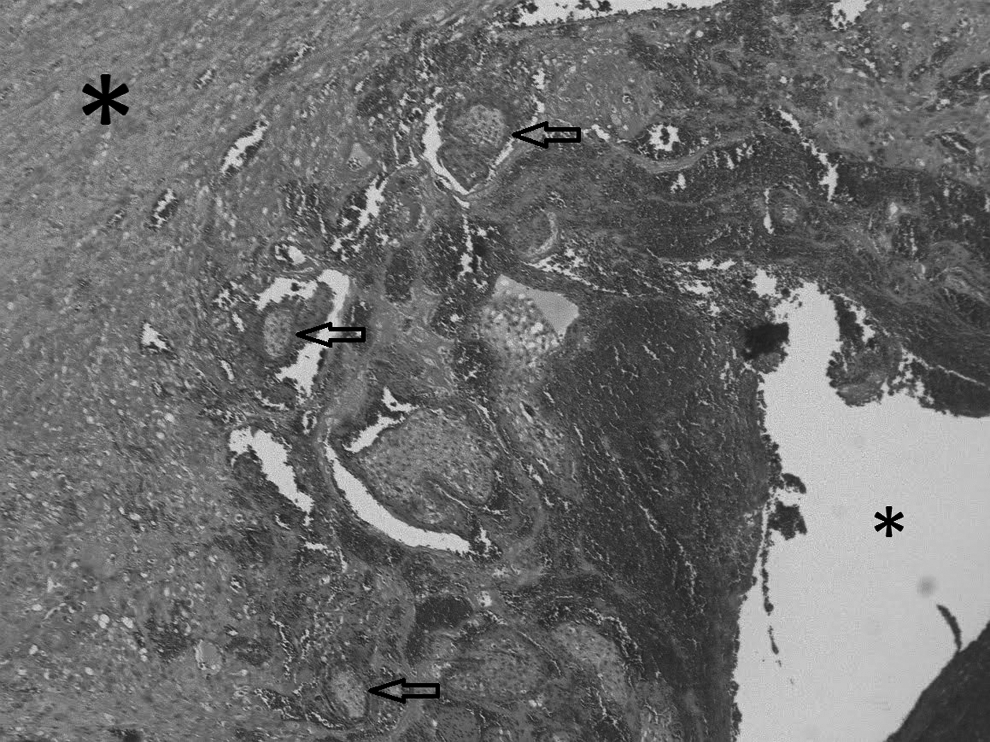
Hematoxylin and eosin microscopy of cervical placenta accreta. Small asterisk indicates the endocervical canal and large asterisk indicates cervical stroma. Arrows show placental villi.
Three days later, the patient was taken to the operating room for the procedure. Upon initiation of suction curettage, a massive uterine hemorrhage occurred. After curettage, an intrauterine Foley balloon, followed by vaginal packing were placed, to control the hemorrhage temporarily. Nevertheless, the patient continued to hemorrhage. Estimated blood loss at this time was between 800 and 900 cc. As she became hypotensive and tachycardic, and the hemorrhage continued, a decision was made to perform an exploratory laparotomy. She was then transitioned to dorsal lithotomy; rapid induction anesthesia was performed; her abdomen was sterilized with Betadine®; and an exploratory laparotomy via a Pfannenstiel skin incision was performed. Simultaneously, the anesthesiologist rapidly transfused 2 units of packed red blood cells, intravenous fluid boluses, and albumin. Upon entry into the abdomen no hemoperitoneum was noted. The bilateral adnexa and ovaries appeared grossly normal, and the uterus was enlarged. The cervix, however, was intact, enlarged, soft, and globular, with a thin window posteriorly, through which products of conception could be seen. Secondary to the unstable status of the patient and continued vaginal bleeding, it was necessary to perform a total abdominal hysterectomy (TAH) in standard fashion, which was performed without complications.
The uterine ligaments were completely detached, and the hemorrhage ceased with ligation of the utero-ovarian and uterine arteries. With the hemorrhage controlled, the uterus was then circumferentially transected at the cervicovaginal junction and the abdomen was closed in standard fashion. During the procedure, the thin window that covered the cervix ruptured, revealing placental tissue. This patient's total estimated blood loss was 1100 cc. Postoperatively, she was hemodynamically stable, did not require further blood products, and was discharged to go home on postoperative day 3 in a stable condition.
Results
Pathologic examination of the cervix revealed placental tissue adherent to endocervical stroma consistent with an intracervical pregnancy with placenta accreta, as well as the corpus uteri containing secretory endometrium with stromal decidualization (Fig. 2).

Transvaginal ultrasound of suspected missed abortion.
Discussion
Placenta accreta is a condition of abnormal placentation caused by trophoblastic invasion into the myometrial tissue beyond the normal boundary established by the Nitabuch fibrinoid layer. 1 Whereas, in normal placentation, placental villi attach to the decidual basalis, microscopic analysis of abnormal placentation has demonstrated partial or complete absence of the decidual layer such that the placental villi attach and/or interdigitate with myometrial fibers.2–7 While other factors such as increased angiogenesis and growth expression may contribute to the pathogenesis of abnormal placentation,7,8 the primary hypothesized etiopathogenesis is via mechanical disruption of the endometrial tissue from cesarean deliveries, myomectomies, uterine ablation, dilation and curettage, or endometritis.2–14 Physiologically, the decidual layer functions as a cleavage line allowing separation between placental cotyledons and the uterus. In the absence of a decidual layer, separation between the uterine spiral arteries and placental cotyledons does not occur, and the uterus continues to perfuse the cotyledons, which, in turn, leads to hemorrhage. 14
Secondary to the rise in frequency of operative procedures (specifically cesarean deliveries, with an estimated incidence increasing from 12.5% in 1982 to 32.2% in 201415–16 ), the current estimated incidence of placenta accreta is 3.0 per 1000 pregnancies. 16 Undiagnosed abnormal placentation can lead to massive intrapartum and postpartum hemorrhage, consumptive coagulopathy, disseminated intravascular coagulopathy, hypovolemic shock, and maternal mortality.2,10,12,13,17,18 Thus, it is becoming increasingly important to analyze placentation antepartum, as well as having a high index of suspicion at the time of delivery. 19
The diagnostic modalities most frequently used are US and magnetic resonance imaging (MRI).20–25 Diagnosis of placental invasion of the myometrium can be made with US, with a positive predictive value (PPV) of 68%, a negative predictive value (NPV) of 98%, and a sensitivity of 89.5% 20 ; with MRI, the sensitivity is 88%, specificity is 100%, PPV is 100%, and NPV is 82%. 21
The case presented was complicated by a cervical ectopic pregnancy with a placenta accreta. Cervical ectopic pregnancy is a rare phenomenon, estimated at <1% of all ectopic pregnancies, 26 while cervical placenta accreta is even more rare, estimated at 1 in 93,000 pregnancies. 12 In comparison to the endometrium, the cervix does not contain a decidual layer; therefore, it is hypothesized that pathogenesis of cervical accretas is attributable to direct damage from cervical instrumentation during dilation and curettage, in vitro fertilization, cesarean delivery, intrauterine device placement, and previous cervical and/or uterine surgery. 9 Risk factors for the current patient were a history of two terminations of pregnancy via dilation and curettage and two lower transverse cesarean deliveries. Over almost the last 2 decades, early diagnosis of cervical ectopic pregnancies via US enabled a trend away from the conventional “gold standard” of TAH toward attempts at preservation of reproductive capacity via intragestational potassium chloride or methotrexate (MTX), local injection of MTX, and prostaglandin F2 alpha, systemic MTX, and/or uterine and hypogastric artery embolization.26–36
For situations when a cervical ectopic pregnancy is encountered, the literature is replete with attempts at conservative management via direct compression (Foley balloon, uterine packing, Blakemore balloon, Bakri balloon), cervical cerclage, mattress sutures, uterine artery embolization, and uterine and hypogastric artery ligation.26–36 Successful management has been demonstrated with single- and multidose MTX therapy with leukovorin rescue, US- and hysteroscopic-guided intra-amniotic MTX injections, and uterine artery embolization.37–42 Patients diagnosed with cervical ectopic and cesarean scar pregnancies have a decreased risk of hemorrhage, hysterectomy, and mortality when treatment modalities, such as MTX, hysteroscopic resection, dilation and curettage, laparoscopy, and laparotomy, are preceded by uterine artery embolization.39,43–48 In the case series presented by Kerns and Steinauer, when confronted with postabortion hemorrhage, 90% of patients treated with uterine artery embolization did not require hysterectomy. 48
However, when conservative measures fail in the acute scenario, one novel solution, as documented by Alammari et al., is vaginal hysterectomy, 49 Another, more-common solution, as in the case presented here, remains the conventional gold standard: TAH.
Conclusions
This case highlights the risks associated with multiple instrumentations of the cervix in reproductive-age women who have undergone multiple terminations of pregnancy. When counseling such patients, the current authors recommend emphasizing the associated risks and potential catastrophic outcomes of a procedure considered by most patients to be innocuous.
Footnotes
Acknowledgments
The author would like to thank Tatiana Holway, PhD, for editing this case report.
Author Disclosure Statement
Both authors have no financial or commercial interests associated with this publication.