
Abstract
Abstract
Background:
Endometriosis occurring in postmenopausal women is rare.
Case:
A 55-year-old woman with a history of panhysterectomy 10 years ago presented with abdominal swelling and pain for several years. Examination revealed the presence of a huge abdominal mass. Ultrasound and computed tomography scanning with dye revealed the presence of a bilobular retroperitoneal mass. An exploratory laparotomy was performed to remove the mass.
Results:
Histopathologic examination revealed that the mass was an old endometriotic mass. The patient made an uneventful recovery; her postoperative hemoglobin 2 days after surgery was 8.5 g/dL, and she was discharged after 5 days on hematinics.
Conclusions:
Retroperitoneal endometriosis can present unexpectedly years after panhysterectomy. Management of such lesions should include careful preoperative assessment, proper patient counseling about the risks, and multispecialty teamwork to obtain the best outcome. (J GYNECOL SURG 33:207)
Introduction
E
The current study reports an unusual case of a huge retroperitoneal endometriotic mass in a postmenopausal woman 10 years after she underwent panhysterectomy.
Case
A 55-year-old woman presented to the outpatient clinic of the Air-Force Specialized Hospital, in Cairo, Egypt, with progressive abdominal swelling and pain for several years. She gave a history of previous 2 ovarian cystectomies, for ovarian endometriomas, that were performed 17 and 15 years ago, in addition to panhysterectomy, performed 10 years ago, for endometriosis. On examination, it was noted that she had a huge mass with limited mobility near the midline and showing shifting dullness on percussion. Abdominal and pelvic ultrasound (US) testing showed a bilobular cystic lesion, measuring 20 × 20 cm. A computed tomography (CT) scan with dye was used to confirm the findings (Fig. 1), as magnetic resonance imaging (MRI) was not available in this hospital. Considering her history and after discussion with the patient, a decision was made to perform an exploratory laparotomy. Her blood was crossmatched, and she gave her consent for that.
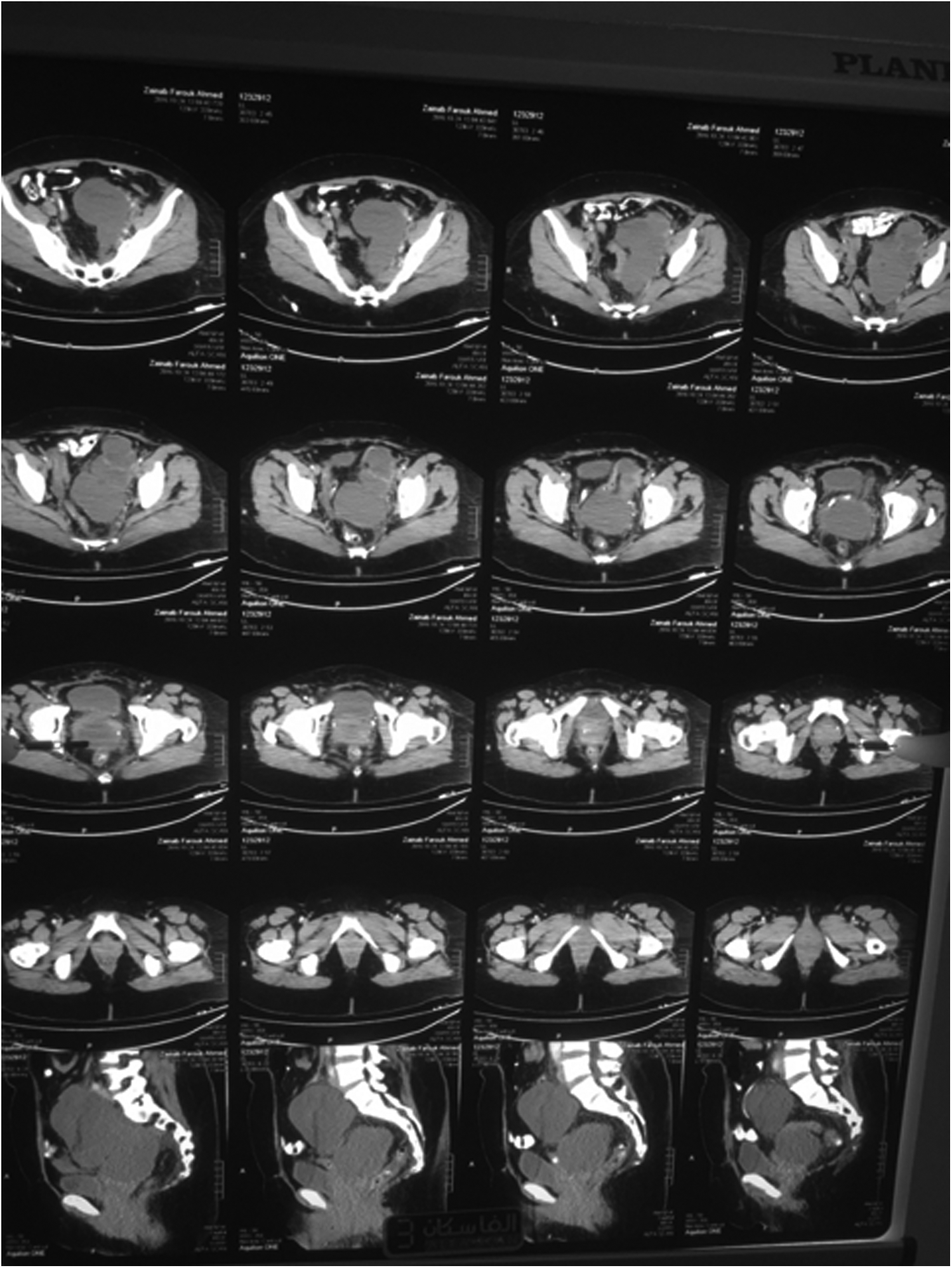
Shows multiple slices of computed tomography scan showing the retroperitoneal mass.
Surgical technique
Through a midline exploratory laparotomy, the abdomen of the patient was explored and a bilobular cystic mass was found, extending between the right and left external iliac arteries. Part of it extended to the edge of the left obturator canal and another part was within the pelvic mesocolon to the other side. The retroperitoneal space was opened and sharp dissection from the sheaths of the external iliac vessels on both sides was performed. Then, dissection from the left obturator canal and through the mesentery of the sigmoid to the other side, with reflection of the mesentery of the sigmoid colon to the other side, was performed until complete excision of the mass was accomplished. It was partly retroperitoneal and partly lateral to the sigmoid colon (Fig. 2). There was no gross evidence of accessory ovarian tissue. The abdomen was closed over a drain, which was removed after 3 days. This patient received 2 units of blood intraoperatively.

Bilobular mass after excision.
Results
The patient made an uneventful recovery; her postoperative hemoglobin after 2 days from surgery was 8.5 g/dL, and she was discharged after 5 days on hematinics. Histopathologic testing showed that she had a huge old endometriotic mass. There was no microscopic evidence of accessory ovarian tissue.
Discussion
Endometriosis is hormone dependent; therefore, it was surprising to find such a large lesion in a patient who had undergone panhysterectomy 10 years prior. However, the current authors think that this mass had started to develop before the panhysterectomy and had enlarged gradually over time, obtaining its blood supply from the great pelvic vessels by attaching to their sheaths, similar to the way parasitic fibroids obtain their blood supplies.
Burney and Giudice 4 and Carvalho et al. 5 provided another explanation for postmenopausal endometriosis, which is the presence of aromatase enzyme responsible for the peripheral conversion of androgens to estrogen in the endometriotic lesions unlike normal endometrium. Badawy et al. 6 proved this explanation by culturing endometrial cells in vitro until maximum growth. The researchers then added testosterone as a substrate for the intracellular aromatase, in addition to an aromatase inhibitor. The researchers evaluated the effect on cell growth and secretion of estradiol and found that testosterone increased the secretion of estradiol by endometrioma cells in the culture, while aromatase inhibitor significantly inhibited the secretion of estradiol and the growth of endometrioma cells. Polyzos et al. 7 and Mousa et al. 8 provided further evidence to support this theory, by showing that treatment of postmenopausal endometriosis with aromatase inhibitors was successful, with the latter study even showing significant reduction in the size of endometriotic lesions in imaging studies.
Preoperative investigations are essential for accurate determination of the distribution of deep infiltrating endometriotic lesions. This is the only way to ensure complete surgical removal. Transvaginal US is among the diagnostic tools for detecting endometriomas; however, its value in the assessment of deep pelvic endometriosis is uncertain.9,10 MRI is frequently used in the diagnosis of endometriomas, 11 as this tool can be used to survey completely both the anterior and posterior pelvic compartments simultaneously. 12 Unfortunately, this imaging modality was not available in the hospital; therefore, the current authors resorted to using a CT scan with dye instead.
Chapron and coworkers 13 proposed a surgical classification that considers the multifocality of lesions during preoperative investigations and surgery for deep endometriosis. This classification is based on the sites of these lesions. These researchers also suggested laparoscopic management for the urinary bladder, vaginal, and uterosacral ligaments with deep endometriotic lesions; and laparotomy for intestinal lesions. The latter involvement was present in the current case, in addition to involvement of the sheaths of the iliac vessels. Ultimately, the large size of the lesion necessitated laparotomy and radical excision of the huge mass.
Radical surgical excision of deep invasive endometriosis lesions is the cornerstone of management for this entity of endometriosis, as medical treatment causes temporarily relief of pain and is associated with a high risk of recurrence after discontinuation of treatment.14,15 Meanwhile, inadequate initial surgery results in progression of the disease, in addition to persistence of pain that may necessitate a second surgery, which is considered both dangerous and difficult.16,17
Surgery for such lesions is not without complications. Kondo and coworkers 18 performed a retrospective study on women undergoing surgery for deep endometriosis at a university hospital in a period over 20 years. The researchers concluded that surgery for deep endometriosis is feasible; however, there is a risk of major complications, especially if rectal surgery is needed. In the current case, the mass involved the pelvic mesocolon, in addition to a different risk of severe bleeding due to the mass' adherence to the great pelvic vessels. Yet, in spite of this, the patient only needed a transfusion of 2 units of blood, which is expected during this extensive surgery. There were no reported complications either intra or postoperative during the patient's stay in the hospital.
Conclusions
Retroperitoneal endometriosis can present unexpectedly years after panhysterectomy. Management of such lesions should include careful preoperative assessment, proper patient counseling about the risks, and multispecialty teamwork in order to obtain the best outcome.
Footnotes
Acknowledgments
The authors would like to thank the hospital staff.
Author Disclosure Statement
The authors declare that they have no conflicts of interest and did not receive any financial support for this case report.