
Abstract
Abstract
Objective:
The main aims of this study were (1) to present prevalence of cytologic abnormal Papanicolaou (Pap) smear, colposcopy results, prevalence of human papilloma virus (HPV) infection in pregnant women, and Pap smear and colposcopy results with histopathology findings 8 weeks after delivery; and (2) the significance of colposcopy in pregnancy.
Materials and Methods:
This was a retrospective study from 2011 to 2012 in the Department of Gynecology and Obstetrics at the University Clinical Hospital Center “Sestre Milosrdnice,” in Zagreb, Croatia. A total of 41 pregnant women were included in the study. Pap smear and colposcopy results during pregnancy and 8 weeks after delivery were analyzed along with HPV testing.
Results:
Pap smears prior to colposcopies showed high-grade squamous intraepithelial lesions (HSILs) in 73% of the women and low-grade squamous intraepithelial lesions (LSILs) in 22%. In 5%, atypical glandular cells (AGCs) seen on colposcopy showed G1 changes in 39% and G2 changes in 46%, and the findings were suspected of being invasive lesions in 5%. High-risk HPV was found in 44% and HPV 16 in 7%. HPV infection was not confirmed only in 5%. Eight weeks after delivery Pap smear showed regression of the disease in 63% and persistence of the disease in 34%. Normal Pap test results were found in 53%. Progression was noted in 3%. Furthermore, on colposcopy-guided biopsy 8 weeks after delivery performed in 15 patients showed LSIL in 13%, HSIL in 67%, and invasive carcinoma in 7%.
Conclusions:
Confirmations were found for high regression rates of Pap smear and colposcopy results after delivery and sufficiency of these tests for detection of cervical carcinoma. (J GYNECOL SURG 33:189)
Introduction
C
Human papilloma virus (HPV) is the most common sexually transmitted infection globally and is responsible for 80%–100% of cervical carcinomas.6,7 Unfortunately, Croatia does not have a national register of patients with HPV infections. In the United States, 50% of the infected population are women ages 15–24, with the highest rate of infection between ages 20 and 30. 8 This is also the reproductive age range when women become pregnant, and most of them have never had gynecologic examinations before, so Papanicolaou (Pap) smears should be obtained during pregnancy. It is also advisable to obtain a Pap smear as part of the routine checkup in early pregnancy, especially if there was no smear obtained in the previous 2 years. 9
Materials and Methods
The aim of the current study was to present the prevalence of cytologically abnormal Pap smear results, colposcopy results, and prevalence of HPV infection in pregnant women treated in the Department of Gynecology and Obstetrics at the University Clinical Hospital Center “Sestre Milosrdnice,” in Zagreb, Croatia. Pap smear and colposcopy results with histopathology findings 8 weeks after the delivery are shown and compared with results in pregnancy.
This retrospective study included 41 pregnant women from 2011 to 2012 at the Sestre Milosrdnice, University Hospital Centre, in whom Pap smear and colposcopy results during pregnancy and 8 weeks after delivery were obtained. These data were analyzed statistically.
Results
Pap smear prior to colposcopy in 41 pregnant women showed high-grade squamous intraepithelial lesions (HSILs) in 73% and low-grade squamous intraepithelial lesions (LSILs) in 22%. In 5%, atypical glandular cells–undetermined significance AGCs-US (Fig. 1) were noted. Colposcopy was unsuccessful in 10%, G1 changes were found in 39%, G2 changes were found in 46%, and the findings were suspected of being invasive lesions in 5% (Fig. 2). HPV testing was performed in 56% of patients. High-risk HPV (HPV-HR) was found in 44% and HPV 16 was found in 7%. HPV infection was not confirmed only in 5% (Fig. 3). Eight weeks after delivery, Pap smears showed regression of the disease in 63% and persistence of the disease in 34% (Fig. 4). Normal Pap test results were found in 53% of patients. Progression was noted in 3%. Furthermore, colposcopy-guided biopsy 8 weeks after delivery performed in 15 patients showed LSIL in 13%, HSIL in 67%, and invasive carcinoma in 7% (Fig. 5).
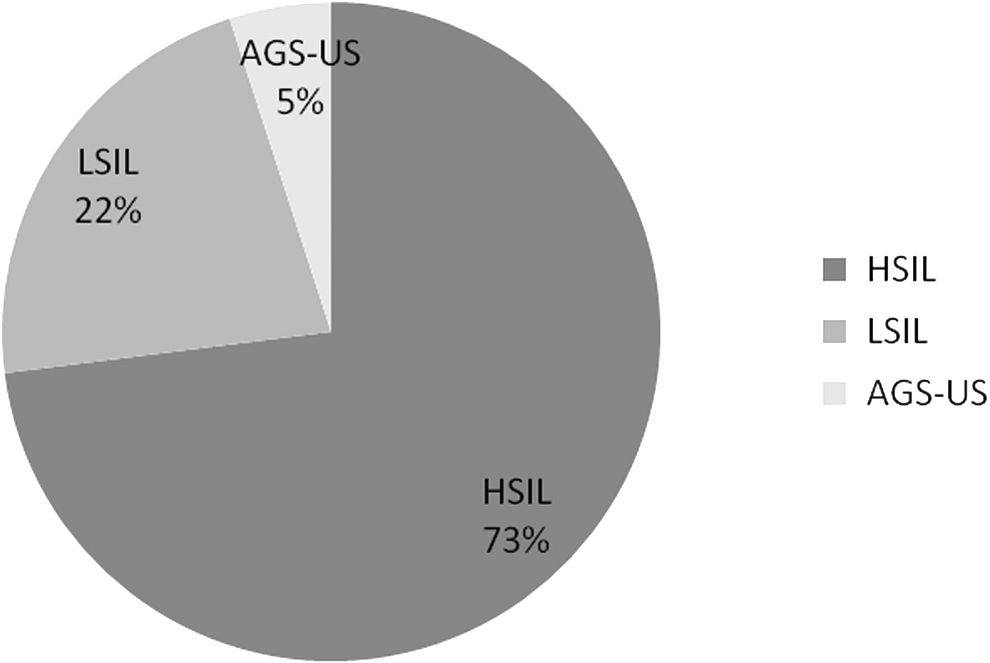
Papanicolaou (Pap) smears in 41 pregnant women in whom colposcopy was performed. HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; AGS-US, atypical glandular cell–undetermined significance.
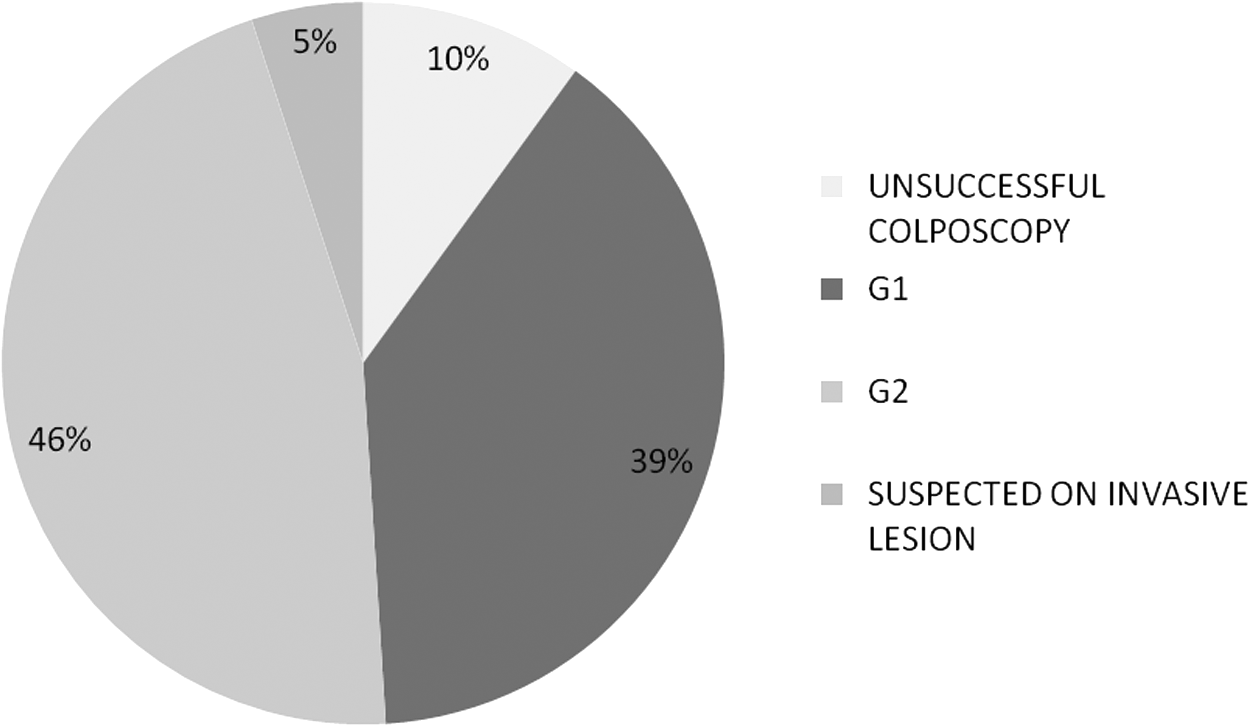
Colposcopy results in 41 pregnant women.

Distribution of human papilloma virus (HPV) in 41 pregnant women.
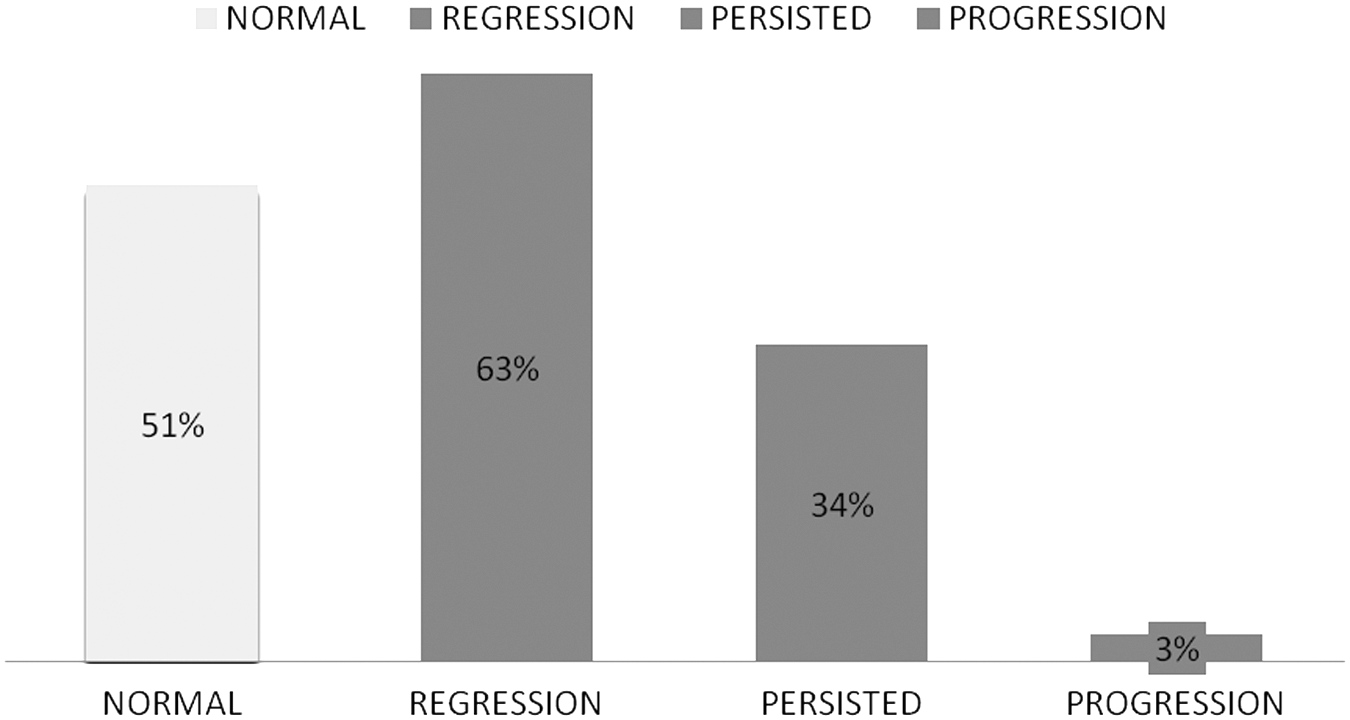
Papanicolaou (Pap) smears 8 weeks after delivery.
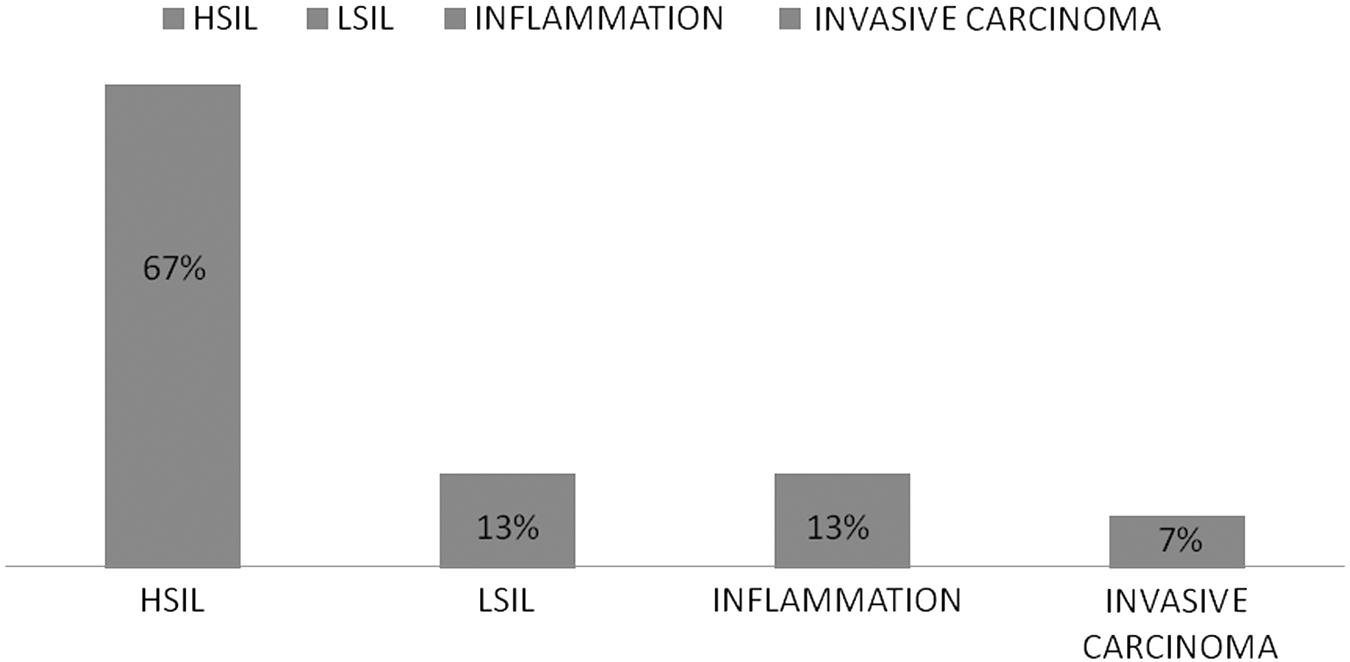
Colposcopy-guided biopsy after delivery. Results for 15 women. HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
Discussion
Management and treatment of cervical premalignant lesions in pregnancy has not been investigated adequately. Most of the studies of cervical lesions are performed in nonpregnant women. According to 2006 Bethesda, MD, guidelines, 10 colposcopy can be postponed after delivery in women younger than age 20 because the risk of HPV infection is high; the rate of abnormal cytology results such as atypical squamous cells–undetermined significance (ASC-US) and LSIL is low; spontaneous regression of these abnormalities occurs in 90%; and there is a low risk of invasive cancer. However, repeated cytology testing is necessary postpartum. In pregnant women older than age 20, management might include further colposcopy evaluation such as that performed in nonpregnant women, but the colposcopy may be postponed until after delivery. In all pregnant women—adolescents or nonadolescents—in whom ASC-H [atypical squamous cells; cannot exclude HSIL], HSIL, or AGC cannot be excluded, colposcopy is recommended. 11
There are no special guidelines for management of cervical pathology in pregnancy in Croatia. Croatia uses the S3 guidelines for nonpregnant woman made by the Croatian Society of Gynecology and Obstetrics with some alterations. 12 If a Pap smear shows ASC-US, the smear should be repeated in 6 months. If ASC-H, LSIL, or HSIL are confirmed, colposcopy must be performed for further evaluation of these changes. Only if an invasive lesion seen on colposcopy is suspected should a biopsy be performed. In case of abnormal colposcopy results—with either minor or major changes—Pap smear with colposcopy should be repeated in 6–12 months.
Such conservative treatment is recommended because during pregnancy cervical intraepithelial neoplasia/squamous intraepithelial lesions (CIN/SILs) are usually stable or regress. 13 Kaplan et al. showed postpartum regression of cervical cytology in 62%, persistence in 32%, and progression to HSIL in 6% in a study of 129 women with LSIL diagnosed in the first trimester. Persistence and progression occurred primarily in women with histories of SILs. 14 Likewise, one large study showed spontaneous regression of HSIL and CIN II and CIN III in 48%–70 % of subjects, and progression to invasive carcinoma in only up to 0.4%.15–17
This improvement of cytology and colposcopy results may be due to a decrease of immunosuppression after delivery, spontaneous regression of SIL, or perhaps trauma during delivery could cause changes in the cervical epithelium.
As previously stated, the main aim of colposcopy in pregnancy is detection of invasive disease in women with Pap smear cytologic abnormalities. Cervical excision is made only if invasive carcinoma is suspected at colposcopy. Pregnancy modifies physiologic findings in the cervix. Vascularity is increased; bleeding after examination occurs more often; and normal eversion of the squamocolumnar junction or benign decidualization can be mistaken for neoplastic lesions. Therefore, the examination should be performed by an experienced colposcopist. Unlike nonpregnant women, in pregnant women, endocervical curettage is not performed because it may disrupt the pregnancy.
Conclusions
High regression rates of Pap smear and colposcopy results after delivery were confirmed. As shown in this current study, because of frequent HPV infections, HPV testing and typization would improve detection of the disease. Cytology testing in combination with colposcopy was sufficient for adequate diagnosis of cervical lesions in pregnancy. Pap smear with colposcopy is the method of choice in detection and evaluation of cervical premalignant lesions during pregnancy. Although such conservative treatment is advisable, recognition of invasive disease should not be missed, and careful postpartum evaluation is necessary.
Footnotes
Author Disclosure Statement
No conflicts of interest exist.