
Abstract
Abstract
Background:
Ovarian hyperthecosis (OH) is a rare cause of hyperandrogenism in postmenopausal women.
Cases:
This article reports 2 cases of postmenopausal women with recent onset hirsutism and androgenic alopecia. Imaging helped confirm an ovarian source of the excess testosterone.
Results:
Bilateral oophorectomy confirmed the diagnosis of OH and led to normalization of serum testosterone. One patient had a unilateral adrenalectomy to remove an adrenal mass with persistently elevated testosterone prior to the oophorectomy.
Conclusions:
Neoplastic sources must be ruled out with respect to hyperandrogenism in postmenopausal women. OH, although uncommon, should be in the differential diagnoses. (J GYNECOL 34:36)
Introduction
T
Ovarian hyperthecosis (OH) is a rarely described cause of hyperandrogenism in postmenopausal women. 2 Affected women typically present with symptoms of virilization of recent onset emulating a neoplastic process. Uncovering the source of the androgen excess is important because of the possibility of malignancy originating from the ovaries or adrenal glands.
Cases
Case 1
A 48-year-old, para 2, menopausal obese woman was referred to the Central Maine Medical Center, in Lewiston, ME, for evaluation of mixed urinary incontinence. At presentation, she was noted to be markedly hirsute. She complained of a 6-month history of progressive facial hair growth necessitating shaving every other day. Her primary care provider had not addressed her hirsutism. She had a history of essential hypertension, insulin resistance, Hashimoto's thyroiditis with nodularity, and recent hospitalization for methicillin-resistant Staphylococcus aureus (MRSA) sepsis.
Her body mass index (BMI) was 34.4 kg/m2 and her blood pressure (BP) was 136/78 mm Hg although she was taking antihypertensive medications. There was pronounced hirsutism on the chest and abdomen, and androgenic alopecia (Fig. 1). A genitourinary examination revealed normal external genitalia and a hypermobile urethra with a negative supine cough stress test. There were no masses noted on bimanual examination but this was limited by her body habitus.

Androgenic alopecia.
An initial laboratory evaluation included levels of: total testosterone, 135 ng/dL (normal range: 9–55); dehydroepiandrosterone sulfate (DHEAS), 56 μg/dL (normal range: 32–240); androstenedione, 0.623 ng/mL (normal range: 0.130–0.820); follicle-stimulating hormone (FSH), 25.9 mIU/mL (premenopausal range: 3–20); and estradiol, 10.1 pg/mL. A transvaginal sonogram revealed the uterus to be 8.2 × 4.9 × 6.6 cm. The endometrial stripe measured up to 0.5 cm and appeared to be homogeneous. The left ovary measured 2.7 × 2.3 × 3.5 cm for a total volume of 11 cm3, and the right ovary measured 2.3 × 1.9 × 2.3 cm for a total volume of 5.2 cm3. No discrete ovarian masses were identified. A computed tomography (CT) scan of the abdomen and pelvis revealed normal adrenal glands without adenopathy. There was some delay in the patient's evaluation and follow-up secondary to transportation and social issues, and, when she was seen, 1 month after initial presentation her total testosterone level had increased to 170 ng/dL.
Because the laboratory findings and imaging were consistent with a nonadrenal source of androgen excess and, despite not identifying a discrete ovarian mass, this patient was counseled regarding a bilateral salpingo-oophorectomy. She missed her preoperative appointment and was seen in the emergency room for myalgia in all extremities. Laboratory evaluation at that time was notable for levels of: thyroid-stimulating hormone (TSH), 94.4 uIU/mL (normal range: 0.400–4.000); and free T4 of 0.6 ng/dL (normal range: 0.7–1.9). She was seen by her primary care provider who referred her to endocrinology. That consultation was delayed by 2 months secondary to social issues. At that visit, another total testosterone level was obtained, which was 318 ng/dL (4 months from initial presentation).
Case 2
A 49-year-old, para 4, menopausal obese woman was referred to the Central Maine Medical Center by her endocrinologist, for a bilateral salpingo-oophorectomy and to address her persistent hyperandrogenism after a recent left adrenalectomy to remove an adrenal mass.
This patient had a history of hypertension, insulin-resistant diabetes, sleep apnea, tobacco use, and hypothyroidism. She had undergone a vaginal hysterectomy 10 years prior for dysmenorrhea. She had presented to her endocrinologist with 6–8 months of rapid progressive facial hair growth, necessitating shaving every other day, and male-pattern baldness.
Laboratory evaluation at that time had included levels of: total testosterone, 209 ng/dL (normal range: 9–55); DHEAS, 29 μg/dL (normal range: 32–240); FSH, 14.5 mIU/mL; and estradiol, 21 pg/mL (menopausal range: 5–38). CT of the abdomen and pelvis revealed a 1.6-cm nodule of the left adrenal gland with characteristics most suggestive of an adrenal adenoma. TVS revealed a surgically absent uterus, a right ovary that measured 3.9 × 2 × 2.7 cm, and a left ovary that measured 4 × 2.5 × 2.3 cm. She was referred to surgery, where she had a left adrenalectomy. Pathology testing of the excised specimen revealed a 2.7-cm left adrenocortical adenoma. Her total testosterone level raised to 258 ng/dL (5 months after her initial evaluation).
At the Central Maine Medical Center, her BMI was 47 kg/m2 and her BP was 174/95 mm Hg although she was taking antihypertensive medications. There was pronounced hirsutism on her face, chest, and abdomen, and she had androgenic alopecia. A genitourinary examination revealed that she had normal external genitalia and a normal urethra. There were no masses noted on bimanual examination, but this was limited by her body habitus.
Results
In both women, laparoscopic bilateral salpingo-oophorectomy was performed uneventfully. Hematoxylin and eosin (H&E) stained sections showed prominent ovarian stromal cells with slightly spindled nuclei and ill-defined cell borders arranged in intersecting bundles with infrequent other residual ovarian elements, such as corpora albicans. Small foci of oval cells with round nuclei and moderate amounts of slightly vesicular cytoplasm were arranged in small clusters and seen within the prominent stromal cells (Fig. 2). These cells are difficult to detect on H&E sections, but react with strong positivity on immunohistochemical stains for calretinin and inhibin-alpha (Figs. 3 and 4).
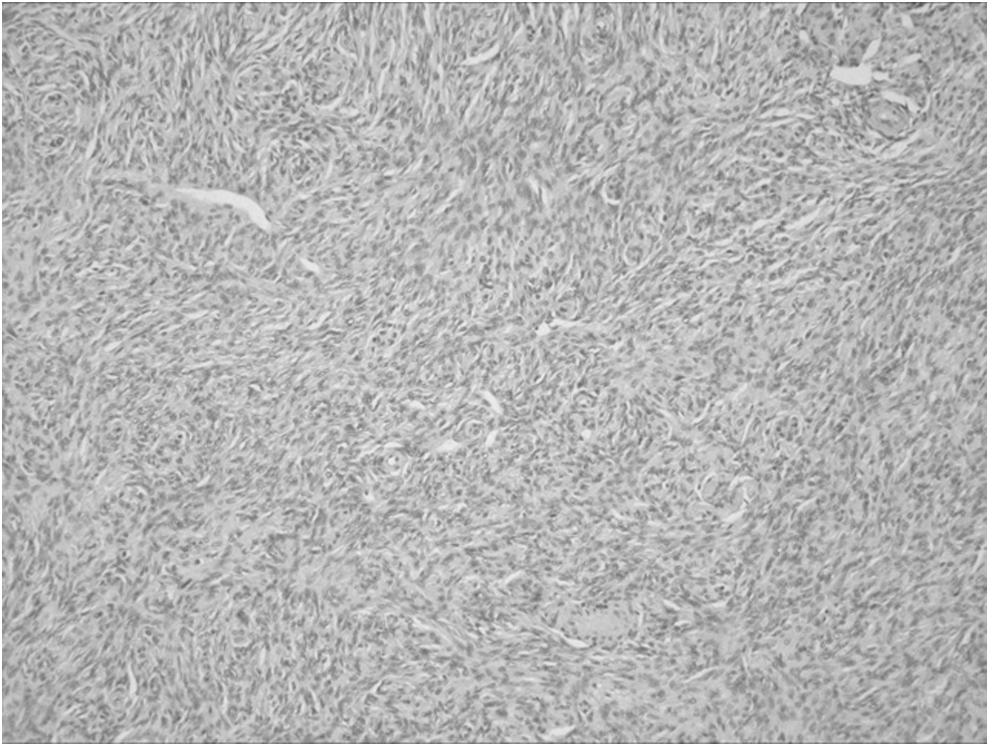
Hematoxylin and eosin staining showed prominent ovarian stromal cells with slightly spindled nuclei and ill-defined cell borders arranged in intersecting bundles.

Calretinin stain at 200 × .
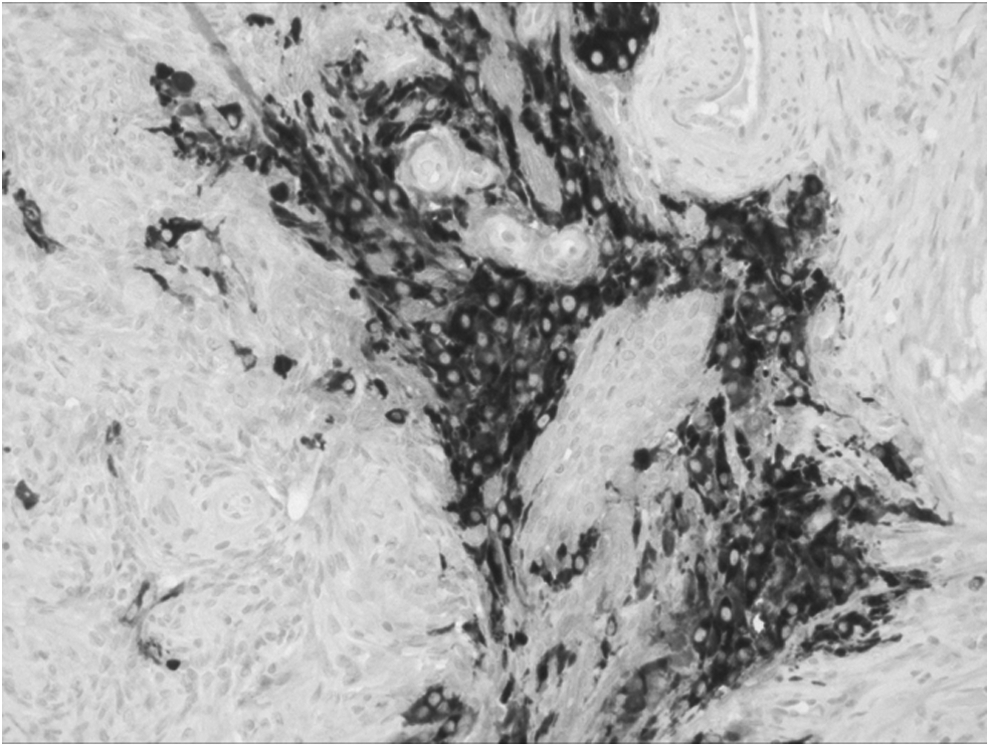
Inhibin stain at 200 × .
Total testosterone 1 week postoperatively was 9 ng/dL and 16 ng/dL, respectively, in cases 1 and 2, and persisted in the normal range. Ultimately, the patients' hirsutism resolved.
Discussion
Despite marked levels of testosterone and ovarian stromal hyperplasia, OH is considered to be a nonneoplastic functional disorder, resulting from disordered regulation of ovarian steroidogenesis, 1 which is rarely reported in postmenopausal women. Both of these patients had normal reproductive histories, central obesity, hypertension, and features of insulin resistance, which is typical of other women presenting with postmenopausal OH. 3 Although the etiology of OH is unclear, it is assumed that insulin resistance and hyperinsulinemia play a role.
Krug and Berga have suggested an algorithm for evaluating postmenopausal hyperandrogenism. 3 Essentially, if DHEAS, total testosterone, and/or 24-hour urinary 17-ketosteroids are elevated, the presence of adrenal tumors must be excluded. The rapid onset of hirsutism and marked elevation in serum testosterone suggested an androgen-secreting tumor and prompted the exclusion of a neoplasm. In Patient 2, that included an adrenalectomy (prior to consultation at the Central Maine Medical Center), which excluded a neoplastic source of androgen excess in the adrenal gland. Alternatively, dexamethasone suppression has been suggested to exclude an androgen-secreting adrenal tumor; if elevated basal total testosterone, DHEAS, and urinary 17-ketosteroids suppress into the normal range with suppression of serum cortisol to <3.3 μg/dL, the likelihood of an adrenal source of androgen excess is low. 4 Patient 2's endocrinologist put her through a dexamethasone-suppression test. This patient's total testosterone had remained high at 223 ng/dL despite cortisol suppression to 2.6 μg/dL. Yet, a decision was made to still proceed with an adrenalectomy.
After laboratory evaluation, imaging is recommended to guide therapeutic intervention in such patients. 3 It can be a diagnostic challenge to discriminate between ovarian virilizing tumors and hyperthecosis. Many androgen-secreting tumors are too small to be seen on ultrasound (US) or CT scanning and, in hyperthecosis, ovarian volume has been reported as either normal or increased. In Patient 1, the CT showed normal adrenal glands and ovaries; on US, it was seen that the patient's ovarian size was, however, increased in relation to her age (11 cm3 and 5.2 cm3), whereas, normal postmenopausal ovaries have a mean volume between 2.5 and 3.7 cm3. 5 Patient 2 also had enlarged ovaries with respect to menopausal status. A common theme in reported cases was the initial misinterpretation of ovarian size being normal if postmenopausal status was not considered. 3 Bilateral ovarian enlargement with an average volume exceeding at least 6 cm5 with elevated testosterone and normal adrenal glands suggests a diagnosis of OH. Most surgeons have moved away from selective gonadal and adrenal venous sampling secondary to complications, including improper catheter placement and adrenal thrombosis and infarction. 6
Bilateral oophorectomy is an effective treatment for postmenopausal women with OH and gonadotropin-releasing hormone (GnRH)–agonist therapy is also given to patients who are otherwise poor surgical candidates or who are unwilling to have surgery,4,7 but these patients are then subject to the side-effects of the therapy. The use of antiandrogens and metformin have not been studied in postmenopausal women with androgen excess.
Conclusions
OH might be difficult to diagnose because ovaries can be misinterpreted as normal size if postmenopausal status is not considered. Ovarian enlargement of at least 6cm3 in the presence of hyperandrogenism and normal adrenal imaging strongly suggest the diagnosis of OH. Neoplastic sources must be ruled out. Bilateral oophorectomy or GnRH agonists are mainstays of therapy.
Footnotes
Author Disclosure Statement
No funding was received for the publication of this article, and there are no relevant commercial interests creating a potential conflict of interest.