
Abstract
Abstract
Background:
Struma ovarii—an uncommon type of benign germ-cell tumor of the ovary—is mainly composed of thyroid tissue. The presence of ascites has been reported in ∼20% of all cases, while a combination of struma ovarii and elevated serum levels of cancer antigen (CA)–125 has been rarely reported.
Case:
A 57-year-old postmenopausal woman presented with a complex pelvic mass associated with ascites and marked elevation of serum CA-125. The clinical impression was ovarian malignancy and she was worked up for staging laparotomy. During surgery, she had total abdominal hysterectomy, bilateral salpingo-oophorectomy, and omentectomy following significant intraoperative findings of 7600 mL of straw-colored ascitic fluid and a right ovarian mass (with both cystic and solid components) measuring 10 cm × 12 cm × 12 cm. A final diagnosis of struma ovarii was made histologically.
Results:
There was an immediate resolution of the ascites and associated normalization of the patient's serum CA-125 level following surgical excision of the pelvic mass. At a 6-month follow-up, she remained free of ascites or tumor recurrence while her laboratory and clinical parameters have also remained normal.
Conclusions:
Clinically, struma ovarii can mimic ovarian malignancy, especially when presented as a complex mass with associated ascites and a high serum CA-125 level. This should be considered when evaluating ovarian masses.
Introduction
A
Although struma ovarii are benign tumors, they can also mimic malignant conditions, such as ovarian cancers, clinically.1,6,7 In a postmenopausal woman presenting with a complex pelvic mass, ascites, associated pleural effusion, and elevated levels of tumor markers, clinical suspicion of a malignant condition would be appropriate. In addition, diagnosing struma ovarii before surgery is difficult, and final diagnosis is usually made by histopathologists postoperatively.4,8 The association of pseudo-Meigs' syndrome and elevated serum levels of cancer antigen (CA)–125 with struma ovarii is an extremely rare condition with the attendant difficulty of differentiating it from a malignancy. In some cases, the tumor produces thyroid hormones with clinical symptoms and, in rare situations, hypothyroidism had been reported following tumor resection.4,8–10 Meigs' syndrome is the presence of a solid benign ovarian neoplasm, especially a fibroma or thecoma, with associated ascites and hydrothorax, which are expected to resolve completely following excision, while, in pseudo-Meigs' syndrome, there are often ascites and pleural effusion caused by pelvic tumors other than fibromas.7,11
Case
Mrs. M.V., a 57-year-old, para 6 (4 alive), postmenopausal woman presented with 3-month history of progressive weight loss and a 2-week history of sudden-onset abdominal distension. There was also an associated history of constipation, early satiety, and loss of appetite. She had been widowed 4 years before presentation and had no clinically demonstrable comorbidities. There were no categorical symptoms or clinical signs to suggest a thyroid-hormone imbalance. On physical examination, it was noted that she was pale but anicteric and had good hydration status despite clinical evidence of significant weight loss. She had no anterior neck swelling and no pedal edema. Her respiratory and cardiovascular systems were essentially normal. Her abdomen was uniformly distended, nontender, and had ascites which was demonstrable by shifting dullness. The intra-abdominal organs were difficult to palpate. Pelvic examination revealed normal female genital structures with associated fullness of the adnexa.
Significant findings on investigations included hypoalbuminemia (3.3 g/dL; reference range: 5.0–8.0 g/dL), an abdominal ultrasound report of complex right ovarian cyst (a 10-cm cyst + a 20-mm solid inclusion with ascites), which was corroborated with the computed tomographic findings (a complex right ovarian mass, most probably malignant, with gross ascites and minimal right pleural effusion), and an elevated serum CA-125 level (3184 μ/mL; normal range: 0–35 μ/mL). Other investigations were reported as being within normal ranges. An assessment of intra-abdominal mass (thought to be most likely an ovarian malignancy) was then made and she was duly counseled on the implications of the diagnosis, pattern, and extent of management including the need for surgical intervention and chemotherapy. She consented to the management schedule and was subsequently worked-up for a staging laparotomy.
Intraoperatively, findings included straw-colored ascitic fluid (7600 mL); a right ovarian mass with an intact capsule (which also has both cystic and solid components), measuring 10 cm × 12 cm × 12cm; and grossly normal left ovary, uterus, and fallopian tubes (Fig. 1). The omentum, bowel loops, liver, stomach, spleen, and diaphragm had no evidence of metastatic deposits. She eventually had total abdominal hysterectomy, bilateral salpingo-oophorectomy, and infracolic omentectomy. She made satisfactory clinical progress postoperatively and was discharged to go home after 6 days.

Gross surgical specimen seen intraoperatively.
Results
The histology was reported as proliferative struma ovarii (Figs. 2 and 3), and she remained clinically stable on follow-up. As of the last clinic follow-up (6 months postsurgery), her investigation results were reported as normal findings on abdominal ultrasonography with normal levels of serum α-fetoprotein (6.5 ng/mL) and CA-125 (22.6 μ/mL; normal range: 0–35 μ/mL). Thyroid function tests were omitted preoperatively as struma ovarii was excluded from possible differentials diagnoses at that time. However, following the diagnosis, these tests were performed and the results were essentially normal.

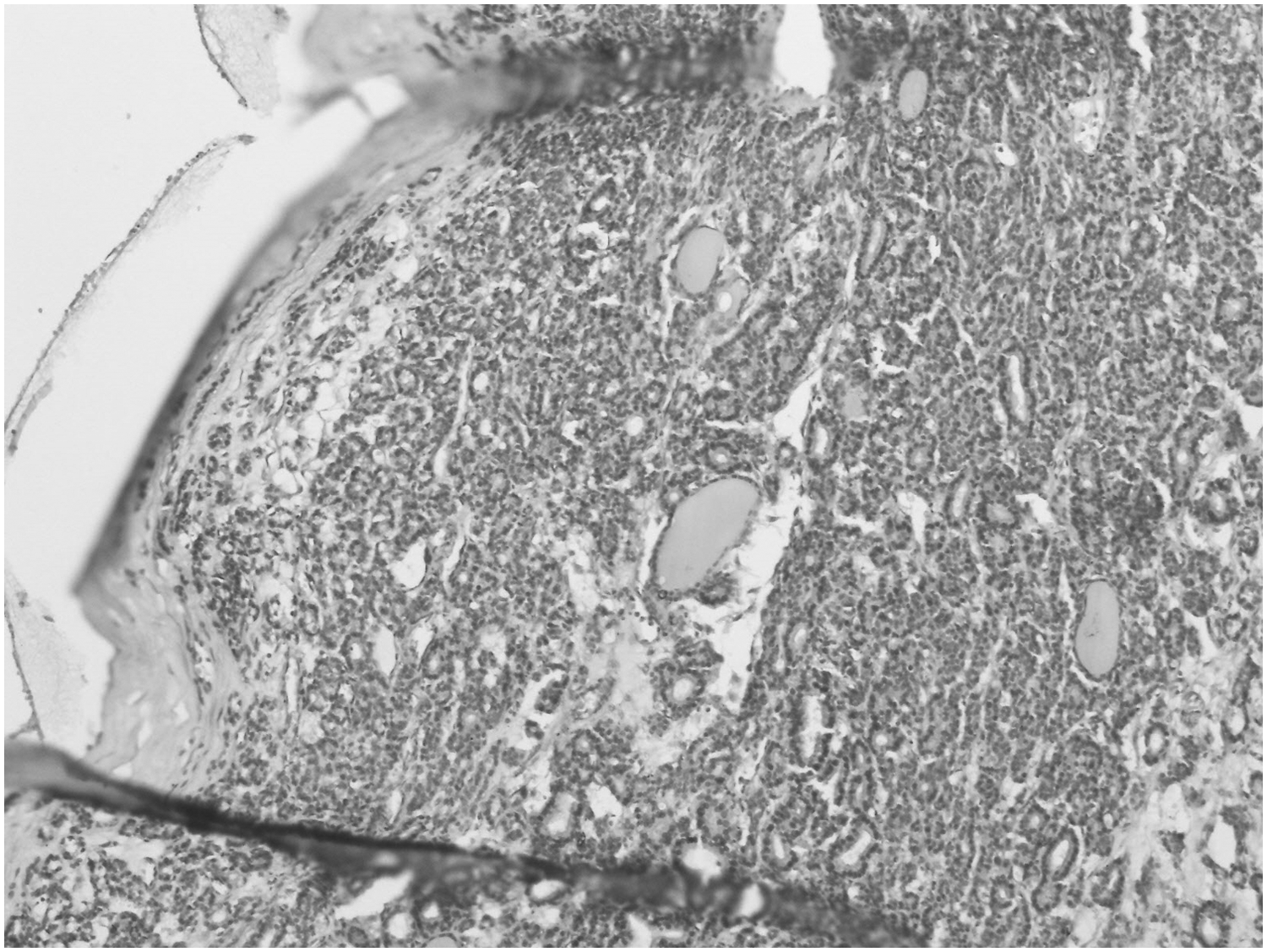
Thyroid tissue (macro- and microfollicular areas) at a higher magnification (hematoxylin and eosin × 400).
Discussion
Struma ovarii, a monodermal variant of an ovarian teratoma, was first described by Boettlin in 1889, when he observed the presence of thyroid follicular tissue in ovaries while further reports were later published by Von Kalden in 1895 and Gottschalk in 1899.1,5,10,12 Although thyroid tissue is generally present in 5%–15% of dermoid tumors, its proportion in struma ovarii should be above 50%.3–5,8,10 Struma ovarii is a benign lesion that can sometimes undergo malignant transformation.3,8 Preoperatively, clinical diagnosis of struma ovarii is challenging because, despite containing a high concentration of thyroid tissue, features of hyperthyroidism has been reported in only 5% of patients with struma ovarii.2–4,6 Although ascites had been reported in one-third of cases, concomitant association with hydrothorax and high serum CA-125 in struma ovarii is uncommon.13–15 Histopathologic examination of the tissue confirms the diagnosis by revealing thyroid follicles filled with eosinophilic colloid. Rarely, associated degenerative changes, such as calcification and fibrosis or hemosiderophages, are reported. 16
Meigs' first described the syndrome, which consists of an ovarian fibroma or thecoma alongside ascites and hydrothorax while the presence pleural effusion and ascites in other benign tumors of the ovary besides fibromas and thecomas was later described as pseudo-Meigs' syndrome.7,11,17,18 The ascitic and pleural fluids in Meigs' and pseudo-Meigs' syndromes are usually serous as in the current patient, but might be serosanguinous and could also be either transudative or exudative. An important factor in the formation of ascites and accompanying pleural effusion is believed to be the tumor size rather than the specific histologic type. 10 Moreover, the actual origin of the effusions has been difficult to describe, although some mechanisms, such as an active tumor, peritoneal fluid secretion, presence of low serum protein, venous or lymphatic obstruction, associated inflammatory products, possible hormonal stimulation, and tumor torsion have been well-described. 1 Overall, few reports have been published on struma ovarii being associated with ascites and elevated values of serum CA125.1,6,7,11,15,17,18
However, significant high levels of serum CA-125 have been reported in many situations involving ascites and pleural or pericardial effusions.1,5,7,10,11,13,15,18 The mechanism of such elevation in CA-125 have been postulated to include peritoneal infiltration by malignant cells or peritoneal stretching by ascites as well as lymphatic absorption of ascitic fluid with a high concentration of CA-125. 10 With respect to possible consequences of peritoneal stretching from ascites in Meigs' syndrome, the serum levels of CA-125 might be elevated, but the degree of elevation hardly correlates with malignancy such that routine measurement in struma ovarii has been said to be of little or no clinical significance.1,5,11 Yet, struma ovarii, as a rare cause of ascites, should be considered as part of the differential diagnosis of a patient presenting with a complex ovarian mass, ascites, with or without pleural effusion and/or high serum levels of CA-125, especially in the presence of negative cytology.6,8,10
Peritoneal strumosis is a benign condition that is often associated with multiple peritoneal implants of varying sizes containing mature thyroid tissue similar to struma and can present with thyrotoxicosis. 19 However, malignant struma ovarii is a rarely seen condition characterized by histologic features of atypia and capsular invasion with high potential for metastasis and recurrence.19–21 Malignant struma ovarii has a poor prognosis similar to other malignant ovarian tumors although thyroid carcinoma metastatic to the ovary should be excluded before diagnosing a malignant struma ovarii.
Generally, presentation with an ovarian mass, ascites, and elevated serum levels of CA-125 in women (especially postmenopausal women) would suggest a malignant clinical condition. Thus, the current case with clinical findings of a large pelvic mass, ascites, pleural effusion, and high serum levels of CA-125 in a postmenopausal woman preoperatively suggested a malignant condition. Following tumor excision and histopathologic investigation, the benign nature of the mass manifested histologically and was followed by complete remission of the ascites and pleural effusion as well as normalization of serum levels of CA-125, thus, requiring no further treatment.
Most previous reports have shown that patients with struma ovarii are largely asymptomatic, or have nonspecific symptoms that are similar to symptoms that occur with other ovarian neoplasms.5,6 In a few circumstances, clinical symptoms, such as a lower abdominal/pelvic mass with or without pain, abnormal vaginal bleeding, ascites, hydrothorax, abnormal levels of thyroid function tests, and, rarely, thyroid tumors can manifest due to the presence of struma ovarii.
Conclusions
This case report of a 57-year-old African woman is meant to strengthen available literature showing that there are benign gynecologic conditions, such as struma ovarii, that could mimic malignancies, based on their clinical, ultrasonographic, and/or biochemical features. Thus, in the differential diagnosis of a complex pelvic mass in a patient presenting with ascites and high levels of serum CA-125 serum, with or without pleural effusions—but with negative cytologic results—the possibility of benign gynecologic conditions, such as pseudo-Meigs' syndrome, should be considered.
Footnotes
Acknowledgments
The author extends thanks to Dr. C.A. Okolo, MBBS, FMCPath, FICS, a consultant histopathologist, at the University College Hospital of Ibadan, Nigeria.
Author Disclosure Statement
The author declares that there are no conflicts of interest.