
Abstract
Abstract
Background:
Microinvasive cervical cancer at International Federation of Gynecology and Obstetrics stage IA1 can be treated with conization or hysterotomy with favorable outcomes. Vaginal intraepithelial neoplasma (VAIN) after hysterectomy for early cervical cancer is sometimes encountered; however, carcinoma in situ (CIS) resulting from VAIN with pelvic cystic formation is extremely rare.
Case:
CIS with pelvic cystic formation occurred 11.5 years after a hysterectomy was performed to treat microinvasive cervical cancer and long-term treatment for persistent VAIN in a 57-year-old multigravida patient. Laparoscopic tumorectomy and adhesiolysis were performed.
Results:
Pathology testing showed CIS. This occurrence was considered to be derived from persistent human papilloma virus infection caused by VAIN. Concurrent chemoradiation was performed, and the patient currently has no evidence of disease.
Conclusions:
CIN or microinvasive cancer can develop subsequent to VAIN even after hysterectomy and can result in progression to cancer. Careful follow-up is the key to early detection of secondary disease. (J GYNECOL SURG 33:219)
Introduction
C
This article reports on such a case and reviews literature about the occurrence of CIS with pelvic cystic formation in early cervical cancer after hysterectomy and long-term treatment of VAIN due to persistent HPV infection.
Case
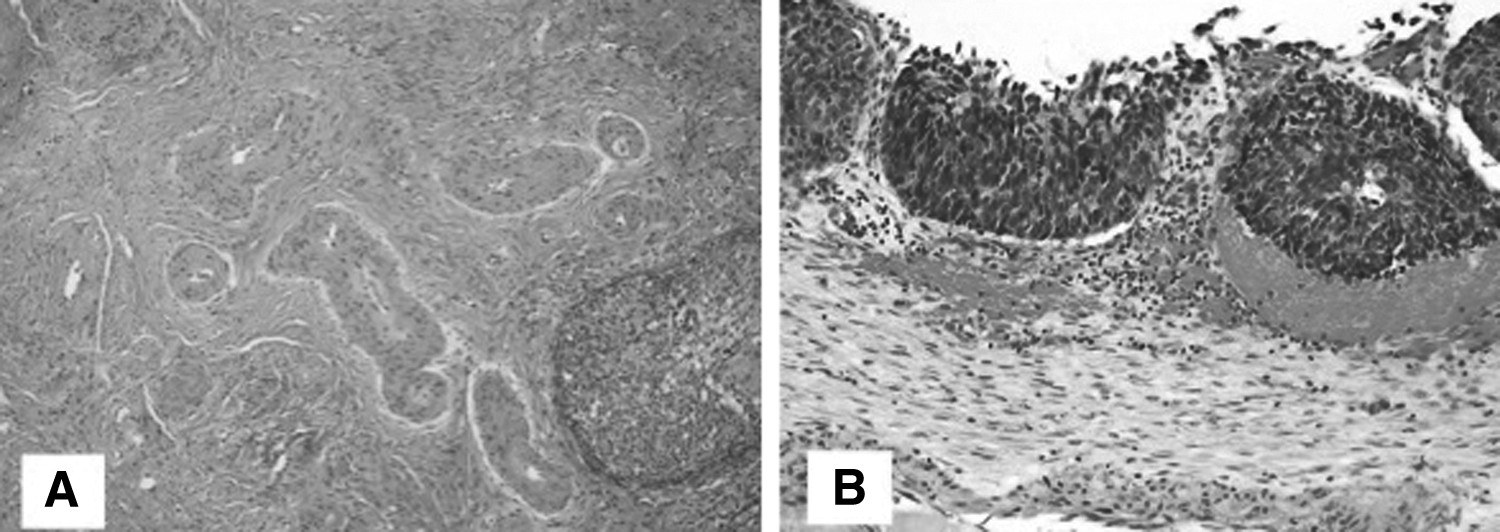
A 57 year-old woman, gravida 3, para 3, was diagnosed with squamous-cell carcinoma according to the results of cervical cell cytology testing and was referred to Chang Gung Memorial Hospital at Linkou, Kweishan, Taoyuan, Taiwan. Cervical biopsy showed the presence of a cervical intraepithelial neoplasm (CIN)3, and conization was performed. Pathologic evaluation showed CIN3 with focal squamous-cell microinvasion without lymphovascular space invasion (LVSI) and CIN3 on the resection margin (Fig. 1A). The result of endocervical curettage was negative for dysplastic cells. One week after the diagnosis, by conization, of FIGO Stage 1A1 cervical cancer, extrafascial hysterectomy and bilateral salpingo-oophorectomy were performed. Histology testing showed carcinoma in situ (CIS) with a negative margin. After treatment, the patient was followed up on a long-term basis as an outpatient, with assessments of vaginal vault smears. Four, six, and nine years after her hysterectomy, laser therapies were performed due to VAIN3 as noted on a vaginal biopsy. All of the lesions were confirmed by colposcopy-guided biopsy.
Three months after the third laser therapy, human papilloma virus (HPV) genotyping showed that she was HPV-66 positive. A vaginal smear was subsequently performed every 6 months and showed normal results. Eleven years after this patient's hysterectomy, a vaginal biopsy showed VAIN1. Eleven and a half years after her hysterectomy, the patient was referred to Chang Gung Memorial Hospital at Linkou, Kweishan, Taoyuan, Taiwan, for abdominal pain. Transvaginal ultrasound and computed tomography revealed an 8-cm cystic pelvic tumor. Her serum CA-125 was 52 U/mL. This was suspicious of a pelvic tumor, which was considered to be the recurrence of VAIN or recurrent cervical cancer; hence, laparoscopic tumor debulking was planned and performed.
Results
Operative findings showed that adhesions were noted among the bladder, peritoneum, and the intestine. A pseudocyst was noted at the cul de sac; this pseudocyst measured 7 cm and had brownish content. Laparoscopic tumor debulking and biopsy of the adhesions were performed. Pathology testing showed CIS (Fig. 1B). Peritoneal washing cytology was positive for malignancy. Concurrent chemoradiation therapy (CCRT) was performed as postoperative therapy. The patient was under intensive follow-up with vault cytology, if indicated, colposcopy, and biopsy with no evidence of disease 27 months after CCRT.
Discussion
The treatment for stage 1A1 cervical cancer is conization or hysterectomy for women who have completed childbearing. Performance of lymphadenectomy is determined by the depth of stromal invasion and LVSI histologically. It is estimated that the 5-year overall survival rate is 95.1% for stage IA1 disease. 2
Predicting factors for residual or recurrent disease after conization is endocervical margin status and presence of high-risk HPV. 3 LVSI is also an independent risk factor for recurrence in patients with stage IA1 cervical cancer. In the current patient, pathology showed stage 1A1 disease without LVSI, which was indicative of a low risk for recurrence. However, she developed intractable VAIN after hysterectomy, following her recurrent squamous-cell carcinoma, with cystic formation. The incidence rate of VAIN after hysterectomy for CIN ranges from 0.9% to 6.8%. 1 In one study of patients who underwent hysterectomy for CIN3, ∼4% had abnormal smears and 0.9% had persistent VAIN lesions. 4 Schockaert et al. reported 1 of 18 (5.5%) patients with microinvasive cervical cancer who developed VAIN3 after hysterectomy. 1 This patient developed VAIN3 10 months after hysterectomy despite having a negative resection margin. Furthermore, a persistent VAIN lesion was present despite repeated laser therapy.
Treatment for VAIN after hysterectomy is laser therapy, vaginectomy, or radiation therapy. Laser therapy has the advantage of being less invasive and causing fewer complications; however laser therapy's success rate is inferior to those of the other treatments. 5 Kim et al. reported that the rate of recurrence after first laser vaporization was 26.5%. Age (< 48 years) and VAIN3 in the vaginal vault before laser vaporization are risk factors for recurrence after laser vaporization. Yet, Ratnavelu et al. recommended conservative surveillance with vaginoscopy and cytology in selected patients with high-grade VAIN depending on each patient's history of previous lower genital cancer and clinical assessment of the lesion. 6 So far, there is no definite management and treatment for VAIN.
With respect to follow-up after hysterectomy for CIN, most researchers have recommended intensive follow-up with vaginal vault cytology, during the 2 years after hysterectomy, to detect VAIN because many cases of recurrence after hysterectomy within 1 year. 7 Once VAIN is detected, long-term surveillance is necessary to enable early treatments and better outcomes.
Late recurrence is defined as >5 years of a disease-free interval and recurrence after 10 years is very rare, 8 especially for very early stage disease. Most recurrences of cervical carcinoma occur within 5 years after the initial treatment, while the incidence of late recurrence is rare (∼1%–3%) and very late recurrence (more than 10 years) is reported to be low, ranging from 0.5% to 0.76%.8,9 The current patient had her recurrence 11.5 years after hysterectomy was performed to treat her microinvasive cervical cancer; the recurrence was detected as a cystic tumor with persistent VAIN despite repeated laser therapy. In this case, the patient's recurrence might have arisen from her VAIN, given that, in her clinical course, this lesion had not vanished despite repeated therapy for it. The recesses in the vaginal apex were incompletely vaporized and left a tract of squamous epithelium hidden in these corners. The squamous epithelium developed into an inclusion cyst with the VAIN persisting.
Conclusions
Persistent VAIN in the vaginal vault may lead to malignant cell proliferation and then tumor formation over many years. In the current case, the vaginal cuff was closed abdominally, which made the risk of leaving intraepithelial disease in the cuff higher. Cystic formation as a recurrence of VAIN is extremely rare. CIN or microinvasive cancer can develop into subsequent VAIN even after hysterectomy and could result in a progression to cancer. Careful follow-up is the key to early detection of secondary disease.
Footnotes
Acknowledgments
The authors thank The Asia-Pacific Association for Gynecologic Endoscopy and Minimally Invasive Therapy (APAGE) for providing the International Fellowship Endoscopy Training Program at Chang Gung Memorial Hospital for Dr. Kusunoki.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.