
Abstract
Abstract
Objective:
By 80 years of age, 11.1% of women are expected to undergo pelvic organ prolapse (POP) surgery and one-third of women are expected to undergo reoperation. The “gold standard” procedure is sacrocolpopexy, which uses a graft to support the vaginal apex to the ligaments of the sacrum. The conventional graft (polypropylene mesh) has been associated with dyspareunia, persistent pelvic pain, and increased mesh erosion. In an effort to combat these complications, a noncrosslinked acellular dermal matrix (ADM; STRATTICE™ Reconstructive Matrix, LifeCell, an ACELITY Company, Bridgewater, NJ) was utilized for this study.
Materials and Methods:
Sacrocolpopexy, with ADM, was used for 9 patients between January 2011 and December 2013. The patients completed Pelvic Floor Distress Inventory-20 (PFDI-20) and pelvic floor impact questionnaires and reported on postsurgical outcome satisfaction. Patient satisfaction with clinical outcomes was assessed. Biopsies of the sacrocolpopexy were performed and tissue samples were sent for histology testing if a patient returned for another procedure.
Results:
During sacrocolpopexy, an ADM was trimmed to fit each patient's anatomy, attached to the vaginal cuff or cervix using sutures, and, when possible, incorporated with the round ligament on each side. The entire sacrocolpopexy was kept in the retroperitoneal space. The postoperative PFDI-20 average score was 25.47 ± 29.68. The postsurgical pelvic floor impact score was, on average, 98%. Patient reported satisfaction with postsurgical outcomes ranged from 70% to 100%. Histology testing showed dense and loose connective tissue with blood vessels, and fibroblast cells and minimal inflammation.
Conclusions:
Other specialties have adopted the use of ADM for defect repairs and breast reconstruction. ADMs can also be used in sacrocolpopexy. (J GYNECOL SURG 33:248)
Introduction
P
Sacrocolpopexy uses a graft to support the vaginal apex to the ligaments of the sacrum. This provides apical support and can correct the anatomical axis of the vagina. 3 The graft material chosen for this operation has been subject to debate. There has been increased litigation with the use of mesh for POP procedures. Patients often cite dyspareunia, persistent pelvic pain, and increased mesh erosion, when their surgeons use conventional polypropylene material.4–6 One of the first sacrocolpopexies performed using a biologic patch was in primates by Rui Liang, MD, and Pamela Moalli, MD, PhD (in a study by Liang et al.) 7 In that trial, a combination of a biologic matrix patch and a synthetic polypropylene mesh resulted in improved tissue ingrowth and a reduced inflammatory response, compared to mesh alone. 7 However, passive mechanical tests indicated that synthetic mesh alone or with a biologic matrix patch were inferior to the nonmesh, nonbiologic matrix patch control. 7 In an effort to combat these complications, physicians are utilizing cadaveric and other nonmesh fascia for sacrocolpopexy procedures. In the present study, a porcine, noncrosslinked, acellular dermal matrix (ADM; STRATTICE™ Reconstructive Matrix, LifeCell, an ACELITY Company, Bridgewater, NJ) was used during sacrocolpopexy.
Materials and Methods
Surgical technique
All patients underwent sacrocolpopexy using a porcine ADM between January 2011 to December 2013. The ADM has been approved for use as a soft-tissue patch to reinforce soft tissue where weakness exists and for surgical repair of damaged or ruptured soft-tissue membranes. This includes body-wall defects, which require reinforcing or bridging material during open or laparoscopic procedures. Each patient was followed up for a 4–8-week postoperative pelvic examination and then for an annual postoperative pelvic examination; each patient had not seen another pelvic floor physician during that time period.
Questionnaires
The patients were seen in an outpatient setting for routine annual pelvic examination. During the examination, pelvic floor measurements—using the stage—urethral hypermobility was performed by a different physician than the one who performed the initial examination and surgery. Additionally, this physician was blinded to the previous preoperative measurements to ensure no bias.
Each patient was asked to fill out a pelvic floor distress inventory (PFDI-20) and a pelvic floor impact questionnaire to assess her subjective degree of satisfaction with her current pelvic floor condition. Low scores on the PFDI-20 are associated with positive postsurgical outcomes. Additionally, the patients were asked to report their satisfaction with the outcomes following surgery. Other data collected included past medical history, past surgical history, preoperative symptoms, postoperative symptoms, and any postoperative complications.
Histology
The high volume of sacrocolpopexies performed in the program at the Women's Hospital Saint Joseph East, KentuckyOne Health, University of Louisville, in Lexington, KY, gives healthcare providers opportunities to see repeat patients when such patients might require a laparoscopy for another reason. Any biopsies collected during the previous sacrocolpopexy were sent to the McGowan Institute for Regenerative Medicine at the University of Pittsburgh, Pittsburgh, PA, for histology testing and unbiased assessment. Histology was performed by Stephen Badylak, MD, PhD, DVM, and the McGowan Institute for Regenerative Medicine. Tissue sections were stained with hematoxylin and eosin as well as a trichrome stain.
Statistical analysis
Descriptive statistics (mean, median, standard deviation, frequency, and percentage) were utilized to examine continuous differences in measurements with the PFDI-20 and the pelvic floor impact score.
Results
Patient demographics
Nine females received sacrocolpopexy with ADM. The average age was 53.67 ± 18.85 years. Common comorbidities included obesity, endometriosis, and gastroesophageal reflux disease (Table 1).
N/A, not applicable; PCOS, polycystic ovary syndrome; IBS, irritable bowel syndrome; GERD, gastroesophageal reflux disease.
Surgical technique
The surgical sacrocolpopexy used an ADM to support the vaginal apex to the ligaments of the sacrum (Fig. 1). The ADM was suitable for sacrocolpopexy, as trimming to fit each patient's anatomy kept it intact. The dermal matrix should not be cut and resutured into a Y-shaped graft, as this is not recommended by the manufacturer and may weaken the dermal matrix at the junction site. The lower portion of the sacrocolpopexy was attached to either the vaginal cuff or the cervix with GORE-TEX® Sutures (W.L. Gore & Associates, Inc., Flagstaff, AZ). by creating a wide base of interrupted sutures (6 or more) such that tension was diverted from any single suture placed. If possible, the round ligament was incorporated on each side, which added to the lateral disbursement of tension on any single point of the vaginal cuff. Sometimes reinforcement of a very thin vaginal cuff area was necessary before placement of the GORE-TEX sutures. The sacral attachment of the ADM was very similar to previous techniques. Three interrupted GORE-TEX sutures were placed in the anterior ligament of the sacral prominence and were staggered slightly, allowing for lateral disbursement of tension.
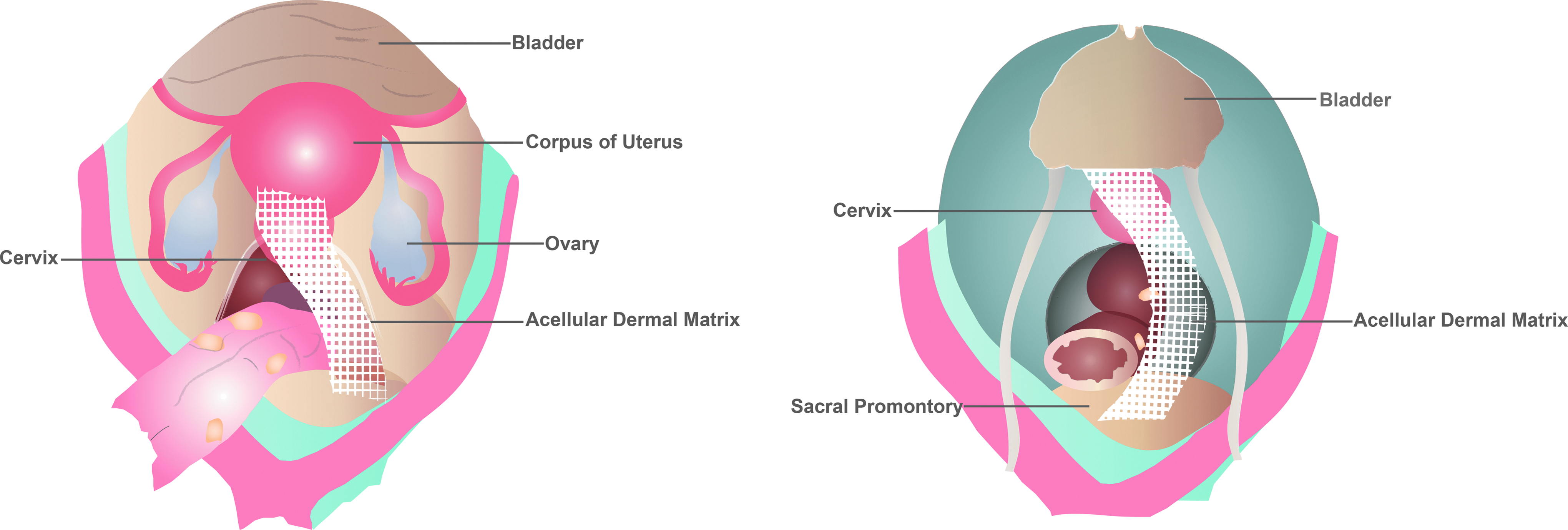
Diagram showing location of an acellular dermal matrix (STRATTICE™ Reconstructive Matrix, LifeCell, an ACELITY Company, Bridgewater, NJ) placement in sacrocolpopexy. Image reprinted with permission from ACELITY.
Reperitonealization to cover the patch completely was a crucially important step. The entire sacrocolpopexy was in the retroperitoneal space when finished, to prevent adhesion formation, to keep the entire healing/regeneration process away from the intra-abdominal structures, and to make future access more accessible with the anatomy visible and identifiable. For the peritoneal closure, a quilted-type monocryl suture was chosen to accelerate the closure process and require less assistance and knot tying.
Questionnaires
The postoperative PFDI-20 average score was 25.47 ± 29.68 (Table 2). The postsurgical pelvic floor impact score was, on average, 98% (Table 3). Patient reported satisfaction with the surgery ranged from 70% to 100%.
POPDI-6, Pelvic Organ Prolapse Distress Inventory 6; CRADI-8, Colorectal–Anal Distress Inventory 9; UDI-6, Urogenital Distress Inventory 6; PFDI-20, Pelvic Floor Distress Inventory.
Histology
One patient returned 1 year later for a separate procedure. At the 1-year follow-up, the ADM was absorbed and the regenerated tissue, located under the peritoneum, was holding the suspension well (Fig. 2). Additionally, histology images showed dense and loose connective tissue with blood vessels and fibroblast cells and minimal inflammation (Fig. 3). The presence of blood vessels indicated good neovascularization. The fibroblast cells were laying down new connective tissue, resulting in tissue regeneration of collagen and ligamentous tissue next to the biologic matrix. Interestingly, there was no foreign-body reaction, dense scar tissue formation, or neoplastic or inflammatory changes.

Intraoperative pictures one year after sacrocolpopexy with an acellular dermal matrix (ADM; STRATTICE™ Reconstructive Matrix, LifeCell, an ACELITY Company, Bridgewater, NJ). The sacrocolpopexy was holding up well with no evidence of adhesions 1 year post surgery. Attachment to the vaginal cuff
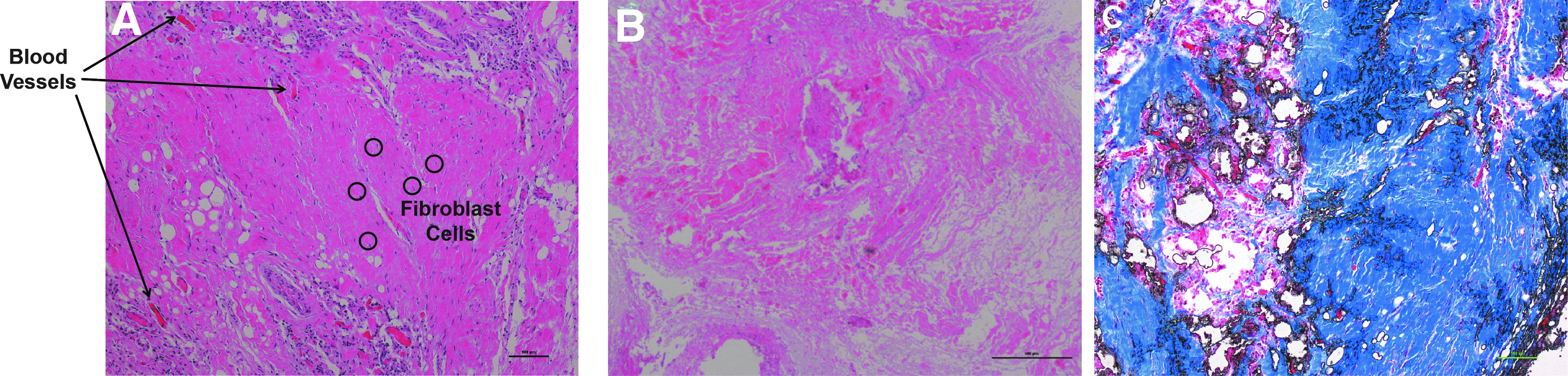
Histology sections from an acellular dermal matrix (STRATTICE™ Reconstructive Matrix, LifeCell, an ACELITY Company, Bridgewater, NJ) sacrocolpopexy biopsy 1 year postsurgery. Blood vessels indicate good neovascularization and fibroblast cells are laying down new connective tissue. No foreign body reaction, dense scar tissue formation, or neoplastic or inflammatory changes are noted. Dense and loose connective tissue with blood vessels and fibroblast cells
Discussion
With the high rates of complications following surgery to correct POP, the pelvic reconstructive program has worked on improving sacrocolpopexy surgery through the use of ADMs. Initially, a porcine bladder source patch was used; however, the uni-sided orientation, difficult handling during suturing, and absorbable properties made this patch completely dependent on the patient's ability to regenerate the tissue next to it—and this would occur only on one side. In certain subgroups of patients (immunocompromised, advanced age, or smokers), tissue regeneration was altered, leading to a less-than-optimal result.
Therefore, a sacrocolpopexy technique was developed that used a porcine ADM. Previously, an ADM with a bilateral orientation that can evoke a tissue-regeneration response (i.e., macrophage migration and neovascularization)8,9 became commercially available. In June 2014, after having numerous positive clinical outcomes, the program switched to using this ADM for laparoscopic sacrocolpopexies and paravaginal defect repairs. To date, the ADM has been used in >150 pelvic prolapse reconstructive procedures.
For optimal results, the ADM was trimmed to fit each patient's anatomy, the lower portion of the sacrocolpopexy was attached to either the vaginal cuff or the cervix with GORE-TEX sutures, and, if possible, the round ligament was incorporated on each side. The sacral ADM attachment was very similar with the placement of GORE-TEX sutures in the anterior ligament of the sacral prominence to create lateral tension disbursement. To achieve the most optimal results, the entire sacrocolpopexy should be located in the retroperitoneal space when the procedure is finished. In the current program's experience, this prevents adhesion formation, keeps the entire healing/regeneration process away from the intra abdominal structures, and makes future access more accessible, with anatomy visible and identifiable.
The current program has learned from experience that biologic patches do produce some liquefaction in the process of stimulating macrophage infiltration and neovascularization. 10 This is a sterile noninfectious process, as no organisms were ever isolated from this area and there were no positive cultures. In the program's experience, there is less liquefaction when using the porcine ADM than what occurs with other biologic products.
The questionnaires were used to assess the impact of this technique on patients with pelvic floor prolapse. The initial findings with these questionnaires have been positive, as they have shown overall patient satisfaction with the clinical outcomes following sacrocolpopexy with ADM.
Conclusions
Other specialties have adopted the use of ADMs in “component separation” for hernia and abdominal-wall defect repairs. A human ADM has been gaining attention in breast reconstruction but not in the field of urogynecology. Based on the positive outcome in the current study, there is a future for the use of ADMs in sacrocolpopexy.
Footnotes
Author Disclosure Statement
Dr. Karon is an unpaid consultant for LifeCell.
Acknowledgments
The author thanks Julie M. Robertson, PhD (of ACELITY) for assistance with manuscript preparation and editing. The author thanks Stephen Badylak, MD, PhD, DVM, and the McGowan Institute for Regenerative Medicine, for his expert opinion and processing biopsy slides. Dr. Badylak's fee for service was paid by the author and was not underwritten by any industry. The author also thanks University of Louisville Biostatistics department for assistance with patient questionnaire development.