
Abstract
Abstract
Background:
Laparoscopic power morcellation has revolutionized laparoscopic surgery by facilitating removal of large uterine masses through small incisions. Recently, there has been a debate on the use of this technique in view of iatrogenic dissemination of myoma tissue necessitating further medical or surgical interventions. Despite meticulous retrieval of all pieces and thorough irrigation, some fragments can elude detection, giving rise to disseminated peritoneal leiomyomatosis or disseminated sarcoma in an undetected malignancy. These complications could require reintervention and may upstage the disease in sarcoma, which worsens patient prognosis.
Cases:
This article reports on 2 cases with complications after laparoscopic morcellation. The first patient had port-site recurrence of a leiomyoma, 3 years after laparoscopic hysterectomy for multiple uterine fibroids, when specimen was removed by power morcellation. The second patient underwent laparoscopic myomectomy for fibroid uterus and the specimen was removed by morcellation. She presented 5 years later with port-site and multiple intraperitoneal leiomyomas.
Results:
After thorough investigation, the first patient was operated on laparoscopically but histopathologic examination revealed leiomyosarcoma; however, on follow-up no recurrence was reported. The second patient underwent radical surgery with removal of all leiomyomata, the uterus, and the omentum. There was no recurrence reported in the second patient on follow-up.
Conclusions:
Reducing accidental spread of uterine malignancy and, at the same time, preserving the benefits of a minimally invasive approach requires careful patient selection, counseling of patients, informed consent, and alternative methods of tissue extraction. These methods include contained morcellation. (J GYNECOL SURG 34:31)
Introduction
U
Cases
Case 1
A 48-year-old female, para 1, live birth 1, presented with a complaint of a large lump in the left side of her abdominal wall at port site. She had undergone laparoscopic hysterectomy 3 years prior for a fibroid uterus, from where a specimen was removed with a mechanical morcellator. Histopathology testing had revealed features of a leiomyoma. After that surgery, this patient had been asymptomatic for 2 years, after which she noticed a swelling at the site of the morcellation port. The swelling continued to grow slowly, up to 10 × 8 cm, occupying the left hypogastrium and left lumbar area (Fig. 1A). The swelling was nontender with irregular margins, and her cough impulse was negative over the mass.
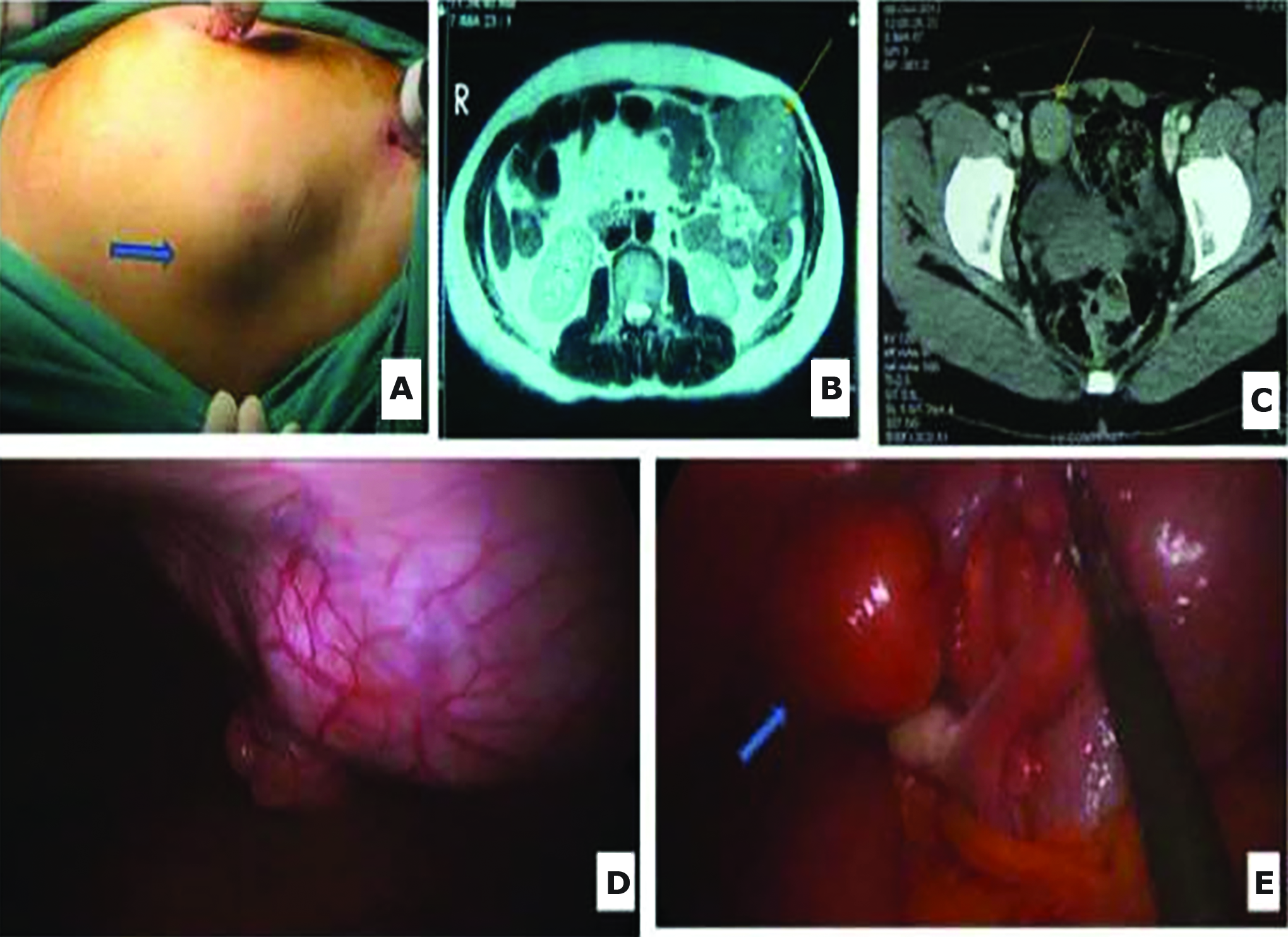
Ultrasonography (USG) revealed a hypoechoic lesion in the abdominal wall involving the rectus sheath, with a provisional diagnosis of a myoma. Fine-needle aspiration of the mass also confirmed the features of a leiomyoma, with tumor cells diffusely positive for smooth-muscle antigen (SMA) and with a very low proliferative index (< 1%). Magnetic resonance imaging (MRI) of this patient's abdomen showed this mass (Fig. 1B) and revealed the presence of another mass ∼4 × 4 cm in the pelvis with similar intensity features (Fig. 1C).
With a provisional diagnosis of a recurrence of this patient's first myoma, diagnostic laparoscopy was planned, which revealed a 3 × 4–cm, round, well-defined pelvic mass near the right infundibulopelvic ligament (Fig. 1D). The rest of the pelvis was normal with normal adnexa. At the site of the larger mass in the abdominal wall, there was 2 × 2 cm of inflammatory tissue attached to the peritoneal side of the abdominal wall (Fig. 1E). The abdomen was opened at the site of the larger mass, and both masses were removed through the same incision.
The patient had an uneventful recovery and was discharged in stable condition after 3 days. However, surprisingly, histopathology testing of both masses revealed features of leiomyosarcoma with high mitotic activity. A positron emission tomography (PET) scan performed immediately after the surgery, and then after 3 months, did not show any abnormality. The patient was followed for the last 40 months and remained asymptomatic.
Case 2
A 34-year-old nulliparous female presented with a lump at a laparoscopic port site, which she had noticed since 1 year prior to presentation. She also had experienced abdominal heaviness for that past year. She had undergone laparoscopic myomectomy 5 years prior for a large 15 × 15 cm, posterior-wall, intramural degenerated myoma. No peritoneal disease was noted intraoperatively during that first surgery. A specimen had been removed with a mechanical morcellator. Histopathology testing of that specimen had revealed features of a leiomyoma with areas of hyalinization, without any evidence of mitotic activity, cellular atypia, or malignant features.
Examination revealed a 5 × 4 cm firm, smooth lump with regular margins at the left port site, and the uterus was enlarged to a 24–26 weeks pregnant uterus size (Fig 2A). MRI of the patient's abdomen and pelvis revealed multiple intraperitoneal masses in the right and left subhepatic spaces, on the right and left anterior abdominal wall beneath the rectus sheath, in the abdominal wall muscle at the left port site, two masses in the pelvis, and one left paramedian mass (Fig. 2B and C). The patient's uterus was also enlarged, with a 10 × 13 × 16 cm intramural myoma. A PET scan also revealed a similar distribution of masses and multiple masses in the mesentery and omentum, raising the possibility of DPL. In the second patient, biopsy was taken from mass attached to anterior abdominal wall peritoneum on right side. Ultrasound-guided biopsy of the mass showed features of a benign smooth-muscle tumor, which was immunopositive for SMA.

Laparoscopy was performed to map the masses, and a biopsy of an abdominal mass also revealed features of a leiomyoma (Fig. 2D and E). Due to the aggressive nature of the tumors, a decision was made to perform complete debulking surgery after obtaining informed consent from this patient. She underwent total abdominal hysterectomy, infracolic omentectomy, and removal of all of the abdominal masses, including a mass attached at the porta hepatis (Fig. 2F). Histopathology testing of all of the masses revealed benign intraperitoneal leiomyomatosis. This patient was followed for 2 years and remained asymptomatic.
Results
The first patient underwent laparoscopic removal of leiomyoma as it was not disseminated. Although histopathology of removed masses revealed leiomyosarcoma the patient remained asymptomatic during follow up. The second patient, however, had a more disseminated disease and hence underwent laparotomy and debulking surgery to ensure complete removal of disease. The second patient was also asymptomatic during follow up.
Discussion
Recently, there has been a debate on the use of power morcellators for tissue extraction in cases of laparoscopic myomectomy and hysterectomy performed for large fibroids. Morcellation confers risks dissemination of tumor fragments—either benign or malignant—throughout the peritoneal cavity, which might necessitate further surgical intervention or worsen a prognosis in cases of unintended morcellation of leiomyosarcomas. The U.S. Food and Drug Administration (FDA) therefore had discouraged the use of power morcellators in April 2014. 4 The FDA has recommended informed consent of patients who undergo morcellation after being given clear explanations of the risks of the procedure and a thorough discussion about other treatment options. Lieng et al. reported a very low rate (0.0005) of leiomyosarcoma in women treated with laparoscopy morcellation for presumed benign fibroids and tissue extraction via morcellation. 5 Only 1 case has been reported in the literature of disseminated leiomyosarcoma 3 months after laparoscopic myomectomy and morcellation for specimen retrieval. That initial histopathology report was of a benign leiomyoma, but on a repeat slide review after the patient presented with a disseminated tumor, features of malignant spindle-cell were found in some cells. A core needle biopsy revealed features of leiomyosarcoma. The patient died after 1 week due to extensive metastasis. 3 In contrast the patient discussed in Case 1 presented with two masses (one in her pelvis and the other at her morcellation port site), which might have been caused by remnants of myoma tissue at the time of initial surgery undergoing sarcomatous changes. Given that this patient had limited dissemination of disease in contrast to the case by Anupama et al., 3 this explains the good prognosis in Case 1. There are two possibilities: (1) Either the remaining pieces of benign leiomyoma transformed into leiomyosarcoma over 3 years; or (2) these pieces had components of leiomyosarcoma already, which were left in place at the time of the first surgery. The second explanation is unlikely because the masses grew very slowly.
There is no reliable preoperative method for diagnosing leiomyosarcoma, and it is usually diagnosed via histopathology testing after surgery for a case of a presumed leiomyoma. In one study, dynamic MRI enhanced with Gd-DTPA [gadopentetic acid] along with serum lactate dehydrogenase (LDH) and LDH isoenzyme 3 seemed to be useful for differentiating a uterine leiomyosarcoma from a degenerated leiomyoma. 6 Leiomyosarcoma must be strongly suspected in a rapidly enlarging myoma or when there are features of degeneration and necrosis, especially in peri- and postmenopausal women.
DPL is a rare benign clinical condition in which multiple smooth-muscle nodules become implanted on the peritoneum of the abdomen and pelvis. Malignant transformation occurs rarely in <5% cases. 7 Van der Meulen et al. performed an extensive literature search of all the parasitic myomas documented in the English-language literature. These researchers reported 69 cases of parasitic myoma after laparoscopic myomectomy or hysterectomy for which specimen removal was achieved via power morcellation. 8 Most of the women presented with symptoms, such as abdominal or pelvic pain, dyspareunia, abdominal distension, urinary frequency, and constipation. Fifteen women (21.7%) were asymptomatic, and the parasitic myomas were diagnosed during either routine examinations or during surgical procedures, performed for other reasons. 8
The incidence of this condition has increased because of iatrogenic seeding of myoma pieces in the peritoneal cavity during morcellation. Siedman et al. identified 1091 instances of uterine morcellation for clinically presumed fibroid uteri. The researchers found unexpected diagnoses of atypical leiomyoma variants or malignant smooth-muscle tumors in 1.2% of cases, with unexpected sarcomas in 0.09% cases. At follow-up laparoscopies of these atypical variants, disseminated disease occurred in 64.3% of all tumors, but only disseminated leiomyosarcoma was associated with mortality. 9 The incidence of atypical variants (including malignancy) is ∼1.2% (0.7%–2.2%) of all morcellated specimens. 10 The risk of occult malignancy at the time of morcellation is ∼1%. 11 Prognosis depends upon the extent of peritoneal dissemination of tissue and the degree of malignant transformation.
Conclusions
The present cases emphasized:
(1) Vigilant examination of the abdomen during morcellation is necessary. (2) Morcellation should be performed by an expert or under guidance. (3) Histopathologic examination (HPE) of every myoma specimen should be performed carefully from each cm of a specimen. Also, specimens from areas of necrosis, degeneration, yellow discoloration, and hemorrhage should be taken for HPE examination. (4) Patients should be given proper counseling regarding chance of atypical variants/sarcoma in the morcellated specimen, leading to all the complications discussed above. The need for follow-ups and repeat surgical interventions should be explained to patients in these special cases. (5) Modified morcellation techniques (i.e., vaginal morcellation, Contained In Bag Morcellation) are emerging as alternative methods of specimen retrieval to avoid intraperitoneal dissemination of the myoma tissue.
12
Footnotes
Author Disclosure Statement
No competing financial conflicts of interest exist.