
Abstract
Abstract
Background:
In patients who undergo hysterectomy for endometriosis, there is the possibility for recurrence. This article, however, reports a rare instance of vaginal cuff endometriosis in a patient who did not have endometriosis prior to her total abdominal hysterectomy (TAH) with a bilateral salpingo-oophorectomy (BSO). The article describes the methodical surgical technique for safe excision of vaginal cuff lesions, with decreased risks to the bladder, ureters, and bowel.
Case:
A 53-year-old female presented with postmenopausal bleeding. She had undergone a total TAH/BSO in 2001 for menorrhagia and uterine fibroids. The operative report described an uncomplicated procedure, and pathology was remarkable for inactive endometrium, adenomyosis, small fibroids, and normal ovaries, without evidence of endometriosis. Since then, the patient had used oral estrogen replacement. On presentation, ultrasonography showed no pelvic masses or fluid collections. She did have vaginal cuff granulation tissue and tenderness on bimanual examination. A vaginal cuff biopsy revealed endometriosis with simple hyperplasia without atypia. The patient elected to have laparoscopic vaginal cuff revision with removal of the vaginal cuff endometriosis that was demarcated by injectable dye as a guide.
Results:
The patient's postoperative recovery was uneventful. No bleeding or pain was noted during a 2-year follow-up period. She was not restarted on estrogen replacement to minimize the risk of recurrence.
Conclusions:
Laparoscopic vaginal cuff revision with the use of injectable dye to ensure complete excision of cuff endometriosis is a feasible and safe method for the management of symptomatic vaginal cuff lesions following hysterectomy. (J GYNECOL SURG 34:92)
Introduction
A
Case
A 53-year-old female presented with postmenopausal bleeding and deep dyspareunia. She had undergone TAH/BSO 12 years earlier for menorrhagia and small fibroids. The operative report described an uncomplicated procedure without evidence of endometriosis, and pathology test results showed inactive endometrium, adenomyosis, small fibroid, and normal ovaries. Since the hysterectomy, the patient had taken systemic estrogen replacement therapy. On presentation, ultrasonography showed no pelvic masses or fluid collections. She was noted to have an erythematous lesion that was initially thought to be vaginal cuff granulation tissue, in addition to a tender vaginal cuff nodule felt on bimanual examination. A vaginal biopsy from the nodule revealed endometriosis with simple hyperplasia and without atypia, rather than granulation tissue. The patient was advised to stop the estrogen replacement therapy and her bleeding subsided 2 weeks later. However, she continued to have deep dyspareunia and a tender indurated vaginal cuff nodule noted on examination. She opted for definitive management with excision of the vaginal cuff nodule.
The operation to resolve the vaginal cuff endometriosis involved laparoscopic enterolysis, laparoscopic vaginal cuff revision, and cystoscopy with ureteral stents placement and removal, performed under general anesthesia with endotracheal intubation.
Laparoscopic trocars were inserted. There was no evidence of endometriosis in the pelvic cavity. Both ureters were near the vaginal cuff as expected. Extensive lysis of abdominal and pelvic adhesions to the anterior abdominal wall, the bladder, vaginal cuff, and the pelvic sidewalls was performed. Dense bladder adhesions to the vaginal cuff were also taken down safely. The bladder was back-filled with saline to identify the bladder boundaries and was subsequently dissected off the vaginal cuff. Using a sterile uterine sound inserted in the bladder can help delineate the bladder wall from the vaginal wall, to minimize the risk of cystotomy and vesicovaginal fistula. The vaginal cuff was easily delineated using a vaginal probe, with distinct separation between the vagina and rectum. A rectal probe was inserted in the rectum to aid with its identification and to rule out rectal involvement with endometriosis or posterior cul de sac obliteration. Neither the rectum nor the rectovaginal septum was involved with endometriosis. The ureters were identified using the ureteral stents. A relaxing incision between the ureter and the uterosacral ligaments was made bilaterally and the ureters were lateralized. The uterine vessel stumps were identified bilaterally to preemptively avoid inadvertent injury and bleeding.
After the vaginal cuff was exposed laparoscopically, speculum examination was performed and revealed a 5-mm nodule in the middle of the vaginal cuff and a deep, tented, and erythematous left vaginal cuff angle, corresponding with the biopsy site and the tender nodule that was felt on bimanual examination. Using a spinal needle and dye, from a vaginal approach, the needle was inserted on both sides of the lesions under laparoscopic guidance. Dye was injected to delineate the desired area of excision, both to ensure complete excision of the lesion (Figs. 1 and 2) and to avoid unnecessary excision of the entire vaginal cuff with associated vaginal shortening and increased risk of injury to the bladder and the ureters. The uterine vessels were dissected and coagulated further along both lateral borders of the planned excision area. An adequate bladder flap was developed carefully. Monopolar energy with a pure cutting current of 60 W was used to circumscribe the area of excision using the dye demarcation as a guide, and an elliptical portion of the vaginal cuff was excised using the vaginal probe as a backstop. Following colpotomy, the erythematous nodule was noted at the left vaginal cuff angle and care was taken to excise the entire area with clear margins to decrease the risk of recurrence and confirm benign pathology.

The desired area of vaginal cuff excision, as determined by the injectable dye and delineated by the dashed-line ellipse.
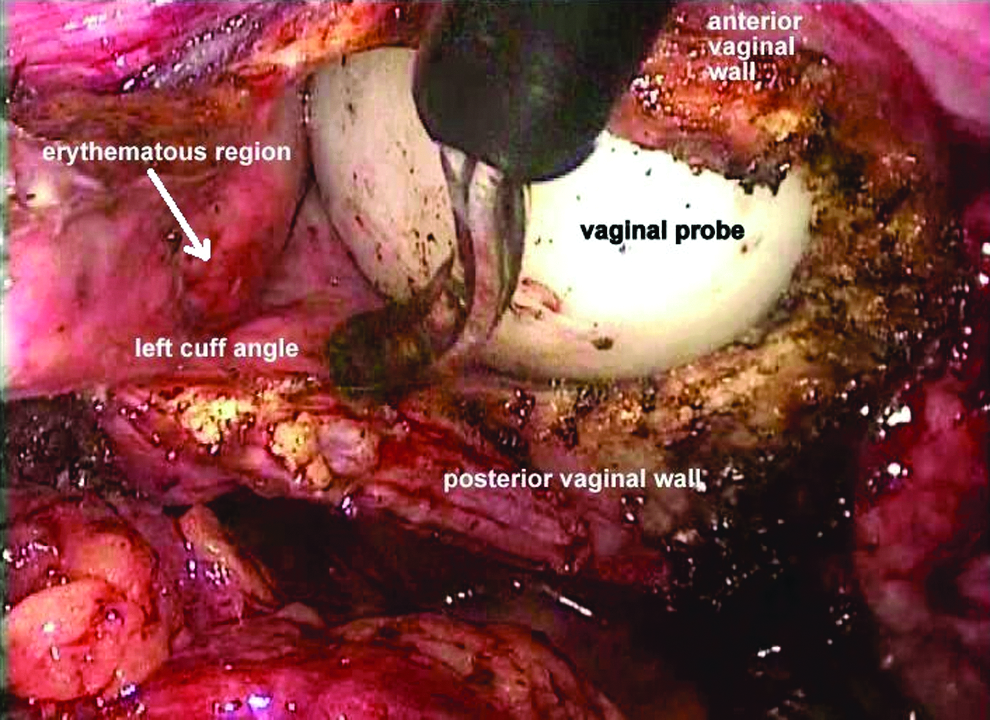
Laparoscopic view of the erythematous nodule at the left vaginal cuff angle (arrow).
The vaginal cuff was closed laparoscopically in the usual fashion with adequate margins to decrease the risk of vaginal cuff dehiscence. Bimanual examination during and at the end of the procedure is very useful when excising vaginal cuff or uterosacral nodules to ensure complete removal of the chronic fibrotic changes surrounding the endometriotic nodule. Cystoscopy was performed after the ureteral stents were removed and normal bladder with efflux from both ureteral orifices was confirmed.
Results
The patient's postoperative recovery was uneventful, and no recurrence of bleeding or pain was noted during a 2-year follow-up period. She was not restarted on estrogen replacement, in order to minimize the risk of recurrence.
Discussion
There is minimal literature examining new-onset endometriosis following hysterectomy. A study from 2011 compared “the incidence of new onset endometriosis after laparoscopic supracervical hysterectomy (LSH) with uterine morcellation to traditional routes,” but the incidence following TAH/BSO was not examined. 3 Another report from 2009 highlighted the potential surgical dissemination of endometriosis following total laparoscopic hysterectomy with mechanical morcellation. 4 This report, however, does not explain the occurrence of endometriosis in the current case, wherein the abdominal approach was used—no morcellation was necessary and no endometriosis was noted at the time of the hysterectomy.
A few theories could explain the pathogenesis of vaginal cuff endometriosis in this patient. The patient did have evidence of adenomyosis—a known risk factor for endometriosis—seen on pathology. 5 Other theories include the possible angiolymphatic spread of endometrial glands, or the rare entity of isolated retroperitoneal endometriosis. 6 Incisional endometriosis may also be considered in this case, similar to incisional endometriosis in cesarean section scars or at the sites of laparoscopic trocars. 7 Furthermore, it is important to note the development of endometrial hyperplasia within this nodule of endometriosis, which was most likely secondary to the prolonged use of unopposed estrogen replacement. 8
There have been studies examining the potential risk of malignant transformation of endometrium with long-term use of unopposed estrogen.8,9 In patients with known endometriosis who require hormone replacement therapy following hysterectomy, there is debate on whether estrogen replacement alone is appropriate versus the need to use combined estrogen–progesterone to avoid the potential deleterious effect of unopposed estrogen on potential residual or recurrent endometriosis.8,10–12
Atypical endometriosis is viewed as being potentially preneoplastic. 13 Although no atypia was found on pathologic examination of the current patient's samples, the only method to rule out a more advanced underlying process is to excise the entire lesion and examine it histologically through complete surgical excision.
Regardless of the cause of the vaginal cuff endometriosis, it is important for the physician to choose the appropriate course of treatment for the patient. Because vaginal cuff endometriosis is rare, there is no standard surgical approach in the literature. While vaginal excision of these lesions is an option, the vaginal mucosal aspect of the endometriotic nodule is often the “tip of the iceberg,” with significant pelvic adhesions that require laparoscopy or laparotomy for proper management. The vaginal approach may also pose excessive risk to the surrounding structures, particularly the bladder, ureters, and bowel, where adhesions are highly prevalent. Rather, choosing to outline the lesions with dye, along with complete laparoscopic excision, should be considered, as this approach provides better visualization and magnification, and allows the safe lysis of adhesions and adequate exposure of the vaginal cuff lesions.
Conclusions
As demonstrated by this case, vaginal cuff endometriosis can develop following TAH/BSO. This may be residual endometriosis that was not recognized or reported during the hysterectomy. This underscores the importance of complete excision of endometriosis, even when hysterectomy and oophorectomy are performed. Despite the paucity of evidence on this rare condition, it is important that physicians are cognizant of this possible long-term development after TAH/BSO and that they recognize that combined estrogen–progesterone replacement therapy could be preferable to estrogen replacement in women with endometriosis. 8 Moreover, if surgical treatment is chosen to resolve the endometriosis, risk to the bladder, ureters, and bowel due to adhesions should be taken into consideration. Removing the lesions laparoscopically and using a dye as a guide provides excellent visualization and allows complete resection of the pathology.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.