
Abstract
Abstract
Objective:
Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome is a congenital aplasia or severe hypoplasia of derivatives of the Müllerian ducts. Various methods of neovaginal creation have been described in the literature, each with its own advantages and disadvantages. This article presents the authors' experience with laparoscopic Davydov's peritoneal pull-through vaginoplasty in a tertiary-care center.
Materials and Methods:
This is a clinical case series of 13 women with MRKH syndrome who underwent laparoscopic Davydov's vaginoplasty in a tertiary-care center from January 2012 to May 2016. The procedure was planned 3 months before marriage. The procedure, intraoperative and postoperative details, and follow-ups of the women are presented.
Results:
Preoperative vaginal length, operating time, and blood loss were 1.38 ± 0.96 cm, 98.61 ± 6.18 minutes, and 33.07 ± 10.31 mL, respectively. There were no conversions to laparotomy; no blood transfusions; and no bladder, ureter, or bowel injuries. Postoperative vaginal length at 6 months was 8.23 ± 1.16 cm. Intercourse was attempted after 97.41 ± 21.84 days postsurgery. All patients had regular follow-ups at 6 weeks, 3 months, and 6 months, and 10 patients reported sexual satisfaction by both partners. Two patients with overall vaginal stenosis and 1 patient with apical stenosis were managed by lateral releasing incisions and a wider mold, respectively.
Conclusions:
Laparoscopic Davydov's procedure is a safe and effective approach for creating neovaginas in women with MRKH syndrome. The procedure has various advantages and confers lowered morbidity on patients. (J GYNECOL SURG 34:63)
Introduction
M
Materials and Methods
This is a case series of 13 patients who underwent laparoscopic Davydov's peritoneal vaginoplasty from January 2012 to May 2016. All women were diagnosed cases of MRKH syndrome with no history of any surgery for neovaginal creation. The procedure was planned 3 months before marriage after obtaining, from each patient, written and informed consent explaining the procedure, associated complications, and postoperative mold usage and regular follow-up. Preoperative bowel preparation was performed for all patients.
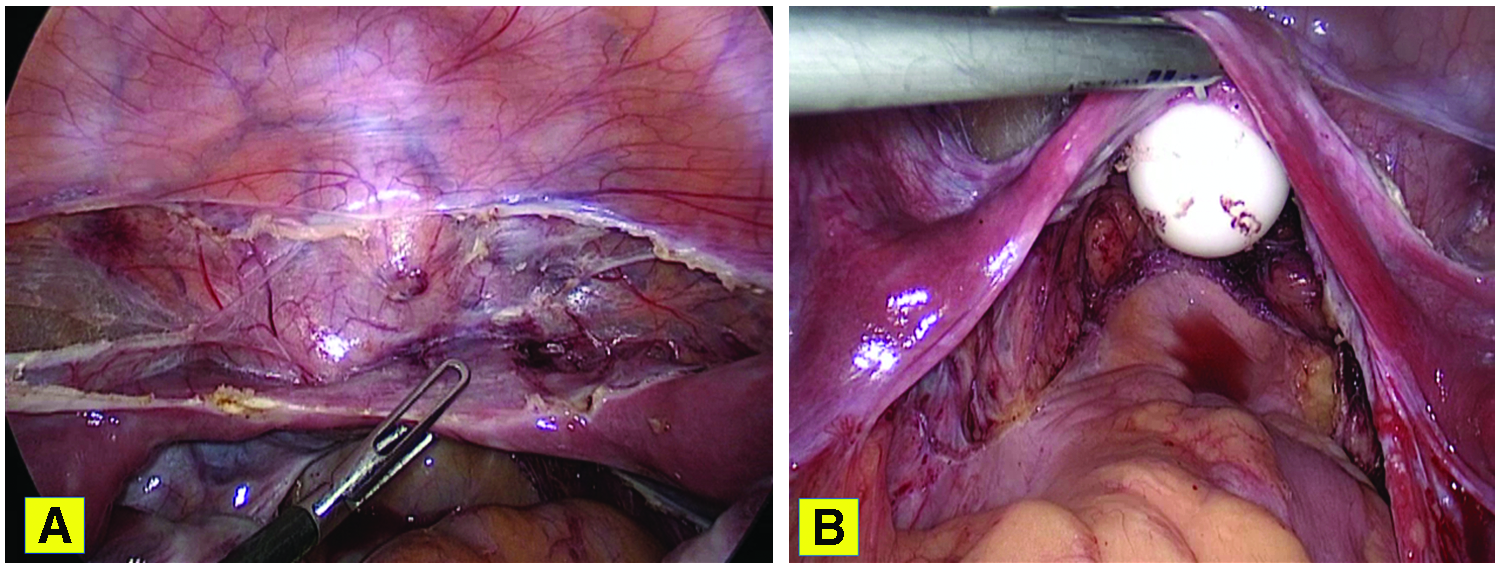
For each patient, the surgery was performed as follows. After general anesthesia, pneumoperitoneum was created with a Veress needle. A 12-mm camera port was inserted 2 cm above the umbilicus and three secondary ports were inserted in such a way that all the ports were in an arc. After laparoscopic anatomical survey, releasing incisions were made over the peritoneum of the lateral pelvic walls medial to the ureters over the assumed position of uterosacral ligaments. The bilateral incisions were made caudally until the vesicorectal septum or Müllerian nodule was encountered. A second peritoneal-releasing incision was made anteriorly just cranial to the bladder dome for better mobilization (Fig. 1). Subperitoneal dissection was performed to free the peritoneum from underlying tissue for easy and better mobilization. Later, vaginal vestibulotomy was performed and a vaginal space was created by using two sets of serial-increasing vaginal dilators and cutting the median raphe with monopolar cautery. The dissection was continued until the glistening peritoneum was reached, with a width accommodating two fingers easily.
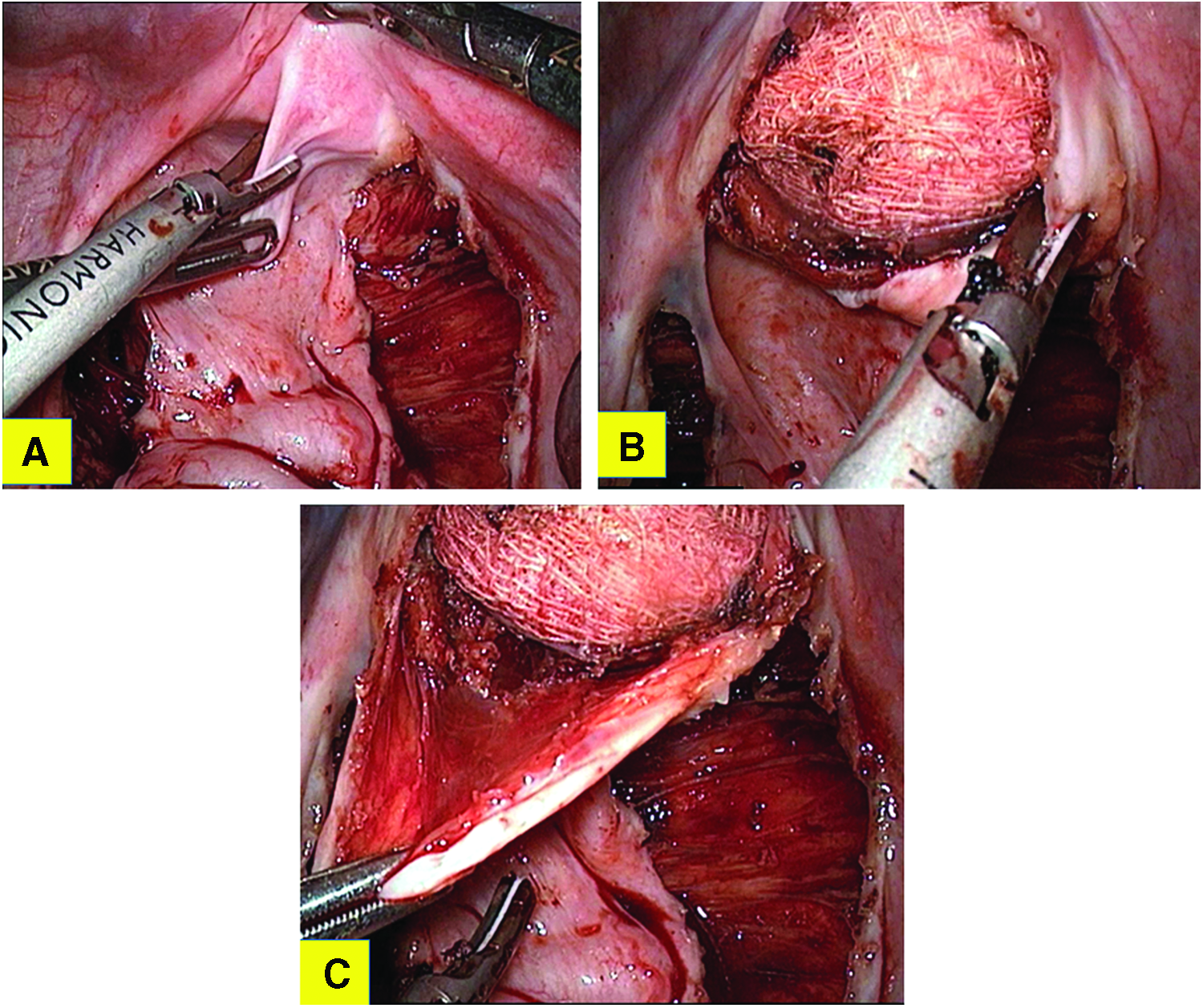
Then, by keeping a sponge on a holder inside the vagina, the vault was opened laparoscopically for a width of ∼4 cm (Fig. 2). The peritoneal edges were brought into the vagina by transfixation sutures to the peritoneum, until the vestibule was reached, and sutured to the vestibule mucosa with interrupted 1-0 Vicryl sutures (Fig. 3). A condom-covered foam mold was inserted into the vagina (Fig. 4). Laparoscopically, a purse string suture with 1-0 Vicryl was used to incorporate the Müllerian remnants on the lateral pelvic wall, the Müllerian nodule anteriorly, the rectal fat posteriorly, and the peritoneum in between these structures to create a vault of a vagina (Fig. 5).
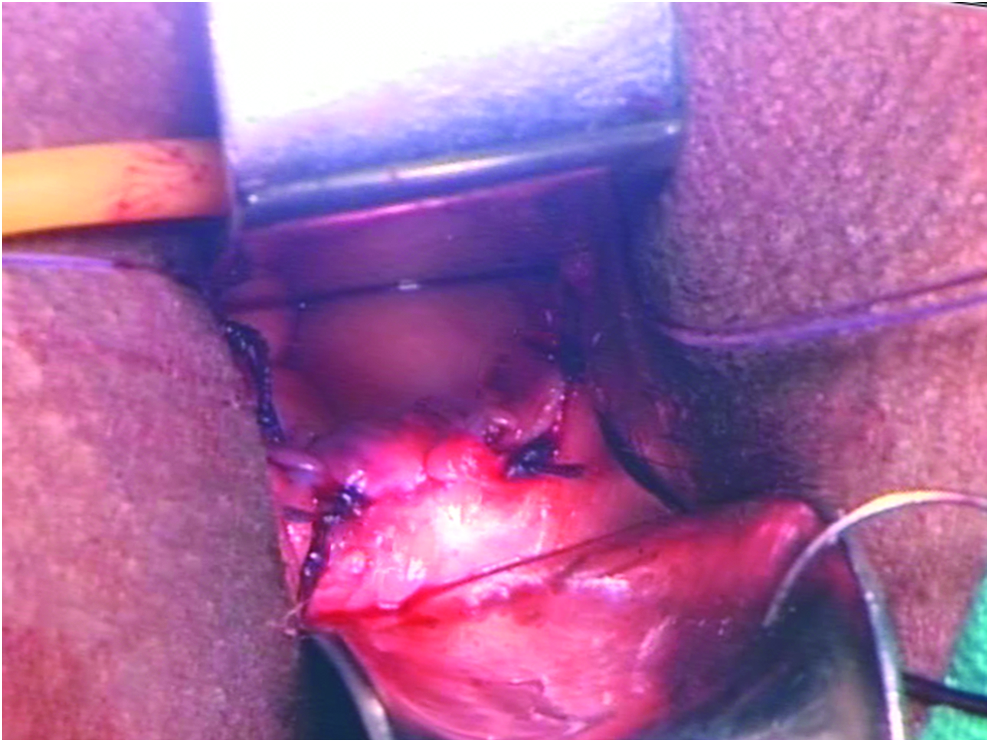
Peritoneum pulled down and sutured to vestibule. Color images available online at www.liebertpub.com/gyn


End view after creating vaginal vault. Color images available online at www.liebertpub.com/gyn
The patient was kept nil per oral for 24 hours. A urinary Foley catheter was retained for 7 days. On the seventh day, the foam mold was replaced by a glass mold. The patient was counseled and taught regarding mold usage, insertion, and sterilization. She was kept under observation for 24 hours and then discharged. Each woman wore a vaginal mold continuously for 6 weeks followed by only night-time mold usage for the next 6 weeks. Follow-up was performed at 6 weeks, 3 months, and 6 months (Fig. 6).

Follow-up speculum examination at 6 months. Color images available online at www.liebertpub.com/gyn
Results
Of 13 women, 10 presented with primary amenorrhea before marriage, 2 presented with dyspareunia after marriage, and 1 presented after a failed dilation method. The mean age of women undergoing the procedure was 21.92 ± 2.05 years. The average preoperative vaginal length was 1.38 ± 0.96 cm. Average operating time was 98.61 ± 6.18 minutes. Average blood loss was 33.07 ± 10.31 mL. There were no conversions to laparotomy. None of these patients received blood transfusions. There were no intraoperative complications and no bladder, bowel, or ureteric injuries. Postoperative average vaginal length at 6 months was 8.23 ± 1.16 cm. Mean duration after which intercourse was attempted was 97.41 ± 21.84 days postsurgery.
Regular follow-ups at 6 weeks, 3 months, and 6 months were completed for all patients. Among 13 women, during follow-up, 2 had overall vaginal stenosis allowing only a width of a finger; this condition was managed by lateral releasing incisions over the vagina with dilation under general anesthesia followed by mold insertion. One woman had constriction at the apex of the neovagina, which was treated by regular usage of a wider mold. The 2 women in whom there was vaginal stenosis were among the initial 5 cases, because the current authors presumed that a mold might not be required during the peritoneal vaginoplasty procedure. However, due to the stenosis that occurred in these patients, a foam mold was kept in situ for initial 7 days, which was changed later to a glass mold for regular daily usage for the rest of the cases. Ten women reported sexual satisfaction by both partners, 2 women reported dyspareunia, and 1 woman was unmarried but using her mold regularly at the time of writing this article.
Discussion
MRKH syndrome is the second most-common cause of primary amenorrhea accounting for 15%. These women are genetic females with normal functioning of ovaries and secondary sexual characteristics but absent vaginas. These patients approach health facilities mainly during adolescence due to an inability to start menstruating or difficulty in having intercourse. Clinically, the main differential diagnosis is androgen-insensitivity syndrome. The treatment goal is to prepare a canal of adequate size for each patient, between the bladder anteriorly and rectum posteriorly, with normal lubrication, when the patient is sexually aroused, to permit sexual intercourse. The neovagina should have intact external genitalia free from scars, stenosis, or contracture, hence, allowing the patient to perform sexual activity satisfactorily. 2
An update on surgical and nonsurgical treatments for vaginal hypoplasia by Callens et al. and the American Congress of Obstetricians and Gynecologists committee opinion states that vaginal dilation should be used as first-line treatment due to its physically low complication rate and an overall anatomical chance of success (vaginal length ≥7 cm) at 75%.3,4 The time required for successful creation of a vagina through dilation ranges considerably between 2 months and 19 months, with the average time in most articles stated as being ∼5– 6 months.5,6 These women usually present as adolescents and might not be emotionally ready to commit to daily dilation. Dilation requires commitment on the part of a patient and it cannot be used to achieve the vaginal length that is possible with a surgical method. 7
Surgery is an option for patients who prefer surgery after thorough informed consent, discussion with their health care providers, and the patients' parents or guardians (for adolescents). 4 There are many surgical methods of creating neovaginas as well as various modifications. For creating a space between the bladder and rectum, form-based or graft-based and traction-based methods are available. 8 Use of laparoscopy provides advantages of minimally invasive surgery to adolescent women. Davydov's peritoneal vaginoplasty and Vecchietti's procedure are two vaginoplasty types that can be performed by laparoscopy with the former being a graft-based method and, later, a traction-based approach. Other graft-based methods are full thickness or split-thickness skin graft, bowel (jejunum, ileum, caecum, sigmoid) graft, and urinary bladder graft.9–12 The principle in Davydov's procedure is the epithelization of the vagina by the patient's own peritoneal graft. In the original Davydov method, peritoneum from the pouch of Douglas was dissected and used as a graft. As time passed, many modifications of mobilizing the peritoneal graft were documented and reported.13–15
The first study comparing laparoscopic Davydov's and Vecchietti's procedures showed significantly shorter hospital stays, less need for postoperative analgesia, early urinary catheter removal, and longer neovaginal length at discharge and at a 12-month follow-up in a group of patients who underwent the Davydov procedure; there was no difference in Female Sexual Function Index (FSFI) scores. 16 Vecchietti's procedure was more time-efficient, but Davydov's procedure was less painful and provided significantly longer vaginal lengths with higher sexual satisfaction. 17 Vecchietti's procedure was also not effective if external genitalia and urethral orifice locations were abnormal. 13
A systematic review by McQuillan in 2014 showed that the longest average vaginal length of 12.87 cm was achieved with bowel vaginoplasty and this was also the most-frequent type of vaginoplasty published in the literature. 7 The same review also showed that the dilation method achieved shortest average vaginal length of 6.65 cm. 7 Bowel injuries are most commonly reported in peritoneal vaginoplasty. 18 Both Frank's dilation method and Davydov's procedure have shown good long-term results, and peritoneal graft can be considered as a good alternative to split-thickness skin graft or sigmoid vaginoplasty. 18
A prospective randomized study comparing laparoscopic-sigmoid with peritoneal vaginoplasty showed significantly less blood loss and shorter operating time in the peritoneal vaginoplasty group. Despite there being no differences in neovaginal length, sexual life initiation time, sexual satisfaction rates, and postoperative FSFI scores between the 2 groups, patients in the sigmoid vaginoplasty group complained of significantly higher (p < 0.005) abdominal discomfort, an unusual odor from vaginal secretions, and vaginal contraction during intercourse. 19
Neovaginal epithelium examined during follow-up after peritoneal vaginoplasty was squamous and had the normal appearance of a vaginal epithelial tissue. 20 This is because of a metaplastic change that occurs in the peritoneum when it is exposed.2,21,22
Thus, the surgical approaches that are available for neovaginal creation have their own advantages and disadvantages. The preferred method has to be decided by the operating surgeon based on his or her experience and expertise. Laparoscopic peritoneal vaginoplasty—in which the homologous graft is the patient's own peritoneum and which has great regenerative and lubrication capacity—has the following advantages over other procedures: There is no risk of hair growth, graft failure, infection, and dehiscence or squamous-cell carcinoma in the vagina. No unsightly scar forms at the harvest site, compared to skin-graft methods. There is no risk of infectious-disease transmission, unlike what can occur in an amnion graft. There is no need for a morbid procedure and associated complications, such as anastomotic leaks and postoperative ileus. There is no risk of adenocarcinoma in the graft. There is no excessive malodorous vaginal secretions, which are known to develop in sigmoid neovaginal procedures. There is no risk of neovaginal prolapse, which can occur in dilation, skin-graft or sigmoid neovaginas. 7 Unlike Vechietti's procedure, peritoneal vaginoplasty can be performed in patients who have had previous unsuccessful vaginoplasties or women with abnormalities of their external genitalia and urethras.13,23 Laparoscopic peritoneal vaginoplasty also does not require placement of a traction device attached to the abdomen, as is the case in Vechietti's procedure. All of these advantages are in addition to the fact that the Davydov procedure can be performed by a minimally invasive route, which is preferred by most adolescent women.
Conclusions
Laparoscopic Davydov's procedure is a safe, feasible, and effective approach for creating neovaginas in women with MRKH syndrome. There are various advantages and lowered morbidity. However, this procedure also requires use of a postoperative vaginal mold during the contractile phase of the wound, which has to be explained to patients before proceeding to this surgery.
Footnotes
Acknowledgments
The authors would like to thank all the residents of the Department of Obstetrics and Gynaecology of the All India Institute of Medical Sciences, Delhi, India, for their collective efforts in data collection.
Author Disclosure Statement
None of the authors have any conflicts of interest to disclose.