
Abstract
Abstract
Objective:
Abnormal uterine bleeding (AUB) is a common symptom for which women seek gynecologic consultations. This study was designed to analyze the endometrial pathologies in patients with AUB and to stratify the incidence of premalignant and malignant changes in these patients, according to their various age groups.
Materials and Methods:
One hundred and ninety-two women, who had AUB, with ages ranging from 23 to 75, underwent endometrial sampling from June 2014 to February 2017 at the All India Institute of Medical Sciences, in Rishikesh, Uttarakhand, India. Endometrial histopathology reports were analyzed.
Results:
The most common clinical presentation was heavy menstrual bleeding (67.2%), followed by irregular menstrual bleeding (28.9%), postmenopausal bleeding (14.5%), intermenstrual bleeding (9.9%), and shortened menstrual bleeding in 2.1%. Women in the perimenopausal-age group (40–50) represented 61.9% (n = 119) and reproductive-age women (23–39) represented 18.2% (n = 35) of the total women. A normal cycling pattern was most common (32.8%; n = 63), followed by disordered proliferative endometrium (28.1%; n = 54). Endometrial polyps were diagnosed in 10.9% (n = 21) of cases. The majority (66.7%) of the endometrial hyperplasia cases were in the perimenopausal-age group (10/15 cases). All of the cases of endometrial carcinoma (n = 3) were in women older than age 50.
Conclusions:
This study showed that the etiology of AUB changes with increasing age and the incidence of premalignant and malignant lesions progressively increase. A significant number of subjects showed underlying organic pathology, especially postmenopausal women, highlighting the importance of endometrial sampling in evaluation. Almost all cases of abnormal bleeding were due to benign causes. This study suggests the possibility of conservative therapy for most cases of abnormal menstrual bleeding. (J GYNECOL SURG 34:12)
Introduction
A
Endometrial biopsy is an important initial diagnostic modality used to assess underlying endometrial changes and, most importantly, to rule out malignancy. This study was carried out to stratify endometrial histopathology in women of various age groups and to analyze the changing patterns with increasing age. About 30% of all hysterectomies are performed following complaints of AUB.3,4 Knowledge of the spectrum of endometrial histopathology can aid in treatment planning and can reduce the number of hysterectomies performed for benign causes.
Materials and Methods
This was a cross-sectional study conducted from June 2014 to February 2017 on patients presenting with AUB in the gynecologic outpatient department at the All India Institute of Medical Sciences, in Rishikesh, Uttarakhand, India. Endometrial sampling was obtained in patients with nongestational AUB, fulfilling one of the following inclusion criteria: (1) heavy menstrual bleeding (HMB) and age >35 years; (2) younger women with anovulatory cycles along with HMB; (3) shortened menstrual bleeding; (4) significant intermenstrual bleeding; (5) HMB with endometrial thickness ≥12 mm on ultrasound (US; Fig. 1); and (6) postmenopausal bleeding.

Ultrasound image showing thickened endometrial lining.
Patients presented with a variety of symptoms, from shortened menstrual bleeding to HMB. The following definitions were used for describing the clinical pattern of bleeding, per the latest terminologies accepted by the FIGO.2,5 The term heavy menstrual bleeding describes the woman's perspective of increased menstrual volume, regardless of regularity, frequency, or duration. 2 Shortened menstrual bleeding is defined as menstrual bleeding of <2 days in duration.2,5 The term irregular menstrual bleeding is used when the onset of menses is unpredictable with a cycle-to-cycle variation of >20 days in individual cycle lengths over a period of 1 year. 2 Intermenstrual bleeding describes episodes of bleeding that occur between normally timed menstrual periods. 2
Based on the above inclusion criteria, a total number of 192 patients for whom endometrial pathology reports were available were included in the study. Endometrial biopsy was obtained in each patient by endometrial aspiration with the help of a Karmann's cannula in the premenstrual phase. All specimens were transported in 10% formalin to the pathology laboratory. The tissue sections were stained with hematoxylin and eosin stain, and microscopic examination was performed by the pathologist. Data on age, parity, presenting symptoms, and the endometrial histopathology report were analyzed and classified into groups. Patients were categorized into 4 groups: group 1, reproductive-age group (ages 23–39); group 2, perimenopausal (ages 40–50); group 3, women older than age 50 who had not attained menopause; and group 4, women with postmenopausal bleeding. Given that the age of menopause in Indian women (average: 44.54 years) occurs at an earlier time than their Western counterparts (average: 50 years), the perimenopausal group was designated as ages 40–50.6,7 Women with AUB who had not attained menopause at an age older than 50 years were considered as a separate group from postmenopausal women with new-onset of bleeding.
Statistical analysis was performed using SPSS IBM, version 20.0. Mean values of continuous variables were assessed using a one-sample t-test. Results were presented as mean ± standard deviation (SD) for age; frequencies and percentages were computed for descriptive variables, such as the type of histopathology reported.
Results
A total of 192 women were analyzed in this study. Their mean age was 44.57 ± 7.89 years. Data on patterns of bleeding were available for 152 cases. There was HMB in 67.2% (n = 102), irregular menstrual bleeding in 28.9% (n = 44), postmenopausal bleeding in 14.5% (n = 22), intermenstrual bleeding in 9.9% (n = 15), and shortened menstrual bleeding in 2.1% (n = 4). The reproductive-age group was comprised of 35 cases, in whom a secretory pattern was the most common finding on histopathology (28.6%; n = 10), followed by disordered proliferative endometrium in 20% (n = 7; Table 1). A subanalysis of the reproductive-age group population, revealed that 10 women were under age 30.
The perimenopausal-age group was the largest, comprising 119 cases (61.9% of total). Disordered proliferative endometrium was the most commonly reported histopathology in this group (30.2%; n = 36), followed by secretory endometrium (24.4%; n = 29) and endometrial polyps in 14 cases (Figs. 2–4). Nine cases each had disordered proliferative endometrium, simple hyperplasia without atypia, and inadequate endometrium.
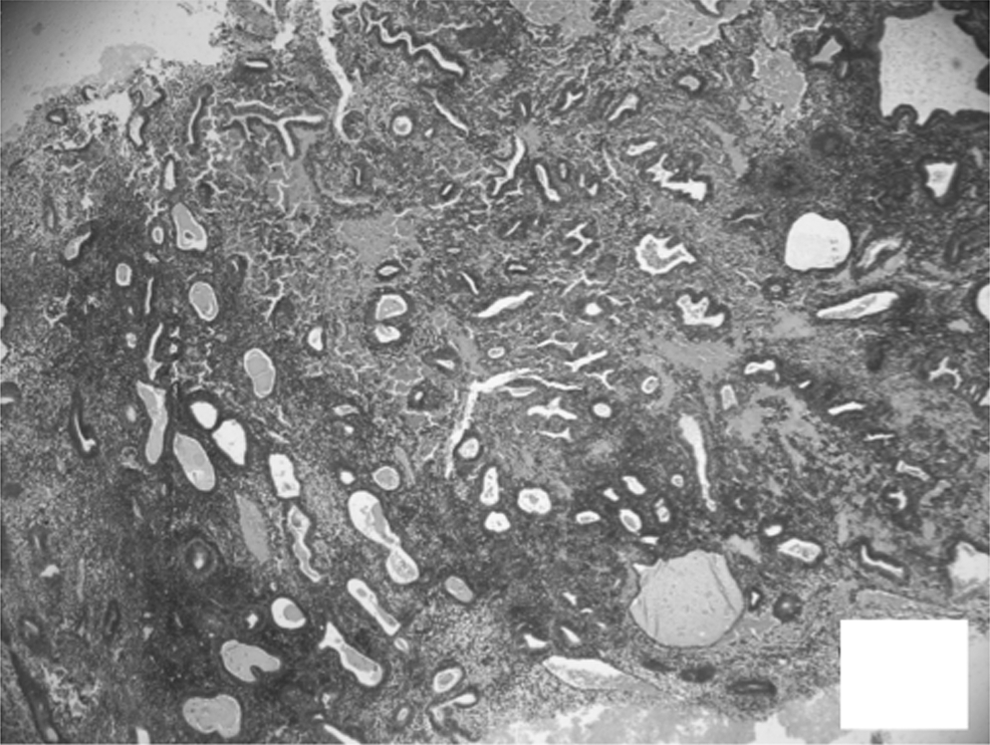
Section from endometrium shows increased number of endometrial glands with crowding and dilatation (hematoxylin and eosin × 20).
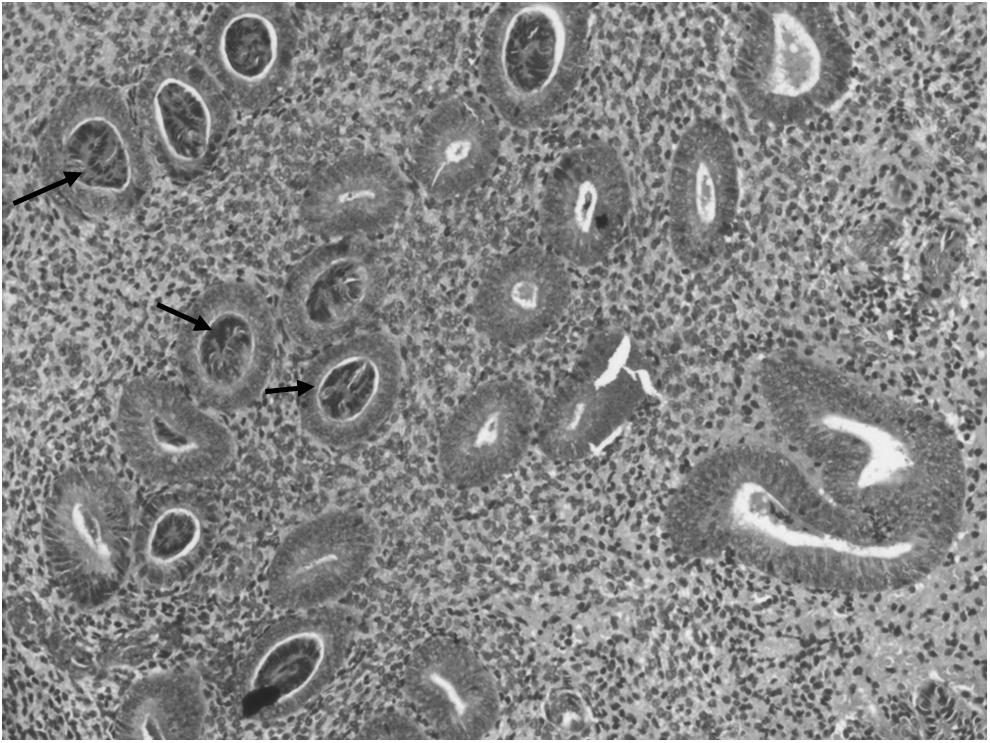
Crowded endometrial glands with some showing gland in gland appearance (arrows). (hematoxylin and eosin × 100).
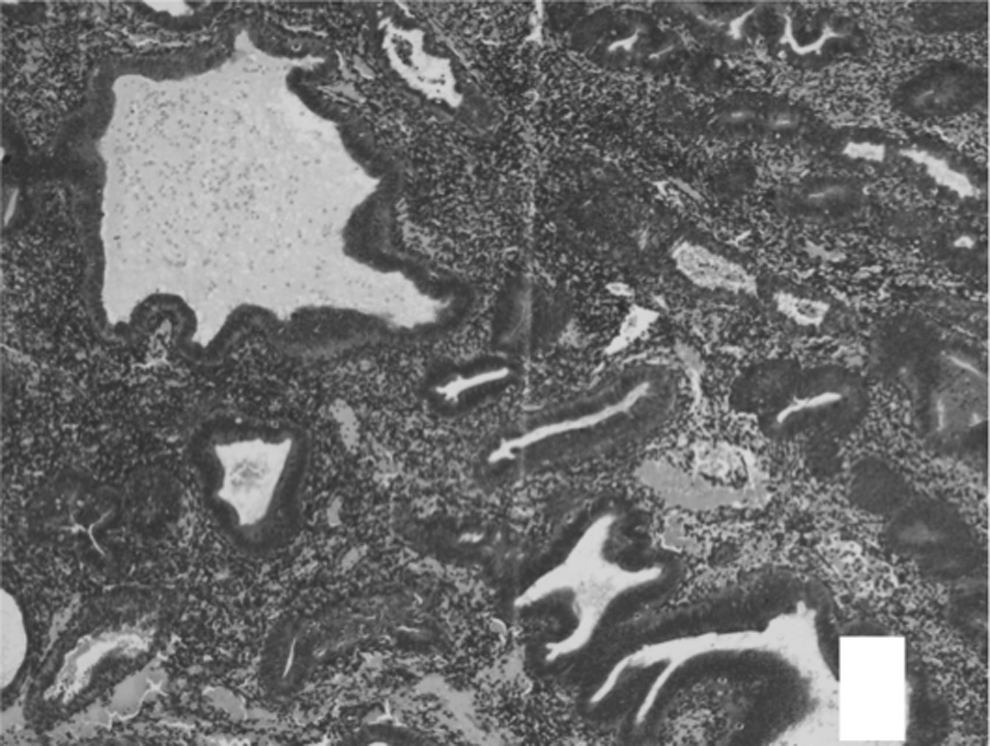
Endometrial glands show pseudostratified lining epithelium, and stroma appears scanty. Endometrial glands show dilatation, outpouching, and infolding (hematoxylin and eosin × 40).
In group 3, the most common pathology was disordered proliferative endometrium (43.7%; n = 7), followed by proliferative endometrium and “pill endometrium” (i.e., endometrium shows changes secondary to exogenous progesterone exposure) in 2 cases each. Adenocarcinoma was found in 1 case in this group. In the postmenopausal group, disordered proliferative endometrium was the most frequent finding (18.2%; n = 4). Endometrial polyps and atrophic endometrium were seen in 3 patients each. In terms of premalignant and malignant changes, 2 patients had simple hyperplasia without atypia, 1 patient had complex hyperplasia with atypia, and 2 patients had adenocarcinomas.
Discussion
Changing patterns of endometrial histopathology were found with increasing age. The youngest patient was age 23. Endometrial biopsy was obtained in her case for HMB with thickened endometrium (22 mm) on US. She was diagnosed as having an endometrial polyp. There were 10 cases under age 30. For most of these patients, a biopsy was obtained in view of anovulatory HMB. Two of these patients had disordered proliferative endometrium, and 1 patient had simple hyperplasia changes. This highlights the importance of endometrial sampling in selected women with anovulatory AUB even in <35 years of age. Two women each had a history of decreased menstrual flow. The histopathology report of 1 of them revealed caseating granulomas secondary to tubercular etiology.
In reproductive-age women of 30–39 years, normal cyclical changes in endometrium were found in 52% (n = 15) of cases. Two cases had inflammatory changes in the endometrium. The overall incidence of endometritis in this study (3.6%; n = 7) was much lower than that reported in other studies (9.1%–13%).8–11 This can be explained by the fact that the reproductive-age group represented a smaller proportion of cases (18.2%; n = 35) in the current study, compared to being the largest one in other studies.9,10,12 The incidence of endometritis in the reproductive-age group was 11.4% (n = 4). Most studies have also found inflammatory changes to be common in the reproductive- and perimenopausal-age groups. This is due to the fact that these changes are induced by spontaneous or surgical abortions and use of intrauterine contraceptive devices, or after exposure to infections such as chlamydial, gonococcal, or tubercular.9,10 Women at reproductive age are more commonly exposed to these causative factors. Doraiswami et al. found a significant group of pregnancy-related complications for AUB in the reproductive-age group 12 (Table 2). These researchers recommended ruling out pregnancy in these ages. However, pregnant patients were excluded from the current study.
The highest number of patients were in the perimenopausal group. Other studies conducted by Muzaffar et al. and Doraiswami et al. have also reported this age group to be the most common population presenting with AUB.11,12 The high occurrence of AUB in this age group can be explained by the physiologic changes occurring prior to the climacteric, which is associated with irregular cycles and periods of amenorrhea followed by heavy bleeding. Normal menstrual changes were the most commonly reported. Disordered proliferative endometrium was the most common reported pathology, which is likely to be due to the anovulatory cycles during the perimenopausal transition. The highest occurrence of endometrial polyps was found in this group (11.7%; n = 14). These polyps are formed secondary to the unopposed estrogen in the anovulatory cycles of perimenopausal women. The prevalence of polyps within a group was highest in the postmenopausal group. Similar to the current study, Behnamfar et al. reported an increasing incidence of polyps in the reproductive- (5%), perimenopausal- (8%), and postmenopausal-age groups (11%). 13
The spectrum of changes induced by unopposed estrogen in women varies from disordered proliferative endometrium to hyperplasia without atypia to atypical changes and finally leading to endometrial carcinoma. Hyperplastic changes were seen in 8.4% (n = 10) of perimenopausal women. There was no case of adenocarcinoma reported in the perimenopausal-age group. Women who do not go into menopause by 50 years of age, can be considered to have abnormal bleeding and are in a high-risk population for harboring premalignant and malignant endometrial changes. Hence, this group was analyzed separately. Disordered proliferative endometrium was the most common finding found in 43.75% (n = 7) of cases in this group. Endometrial adenocarcinoma was found in 1 of the total 16 cases (6.3%).
Few other studies have considered women older than age 50 in the postmenopausal group. However, in the current study, only women who had secondary amenorrhea for at least 1 year and then developed new-onset bleeding were included in the postmenopausal group. The proportion of cases with endometrial hyperplasia was much higher in postmenopausal women (13.6%; n = 3). One of these showed atypical features. Overall incidence of adenocarcinoma (1.5%; n = 3) was similar to that seen in other studies.10,14 All of the cases of adenocarcinoma were found in premenopausal women older than 50 years of age and in postmenopausal women. Atrophic endometrium was found in 5 women (2.6%). Three of these women were in the postmenopausal group. The physiology behind endometrial atrophy is the decline in endogenous hormones after menopause and declining ovarian reserve in perimenopausal women. An incidence of 2.5%–6% for atrophic endometrium has been reported in other similar studies.10,12
In the current study, in the majority of the cases no organic pathology was found. Normal menstrual pattern changes were the most frequent finding. Abnormal bleeding in cases of proliferative endometrium can be explained by anovulatory cycles causing irregular prolonged menses. 12 Patients with secretory endometrium findings present with regular heavy cycles, due to ovulatory dysfunction. 12 Abnormal endometrial pathology was found in only 52.1% of patients in the current study. Most of these cases with abnormal pathology could be managed conservatively, as malignancy incidence was just 1.5%.
Numerous complications are known to be associated with hysterectomy, such as ureteral and bladder (2%) injuries; hemorrhage (1%–3%); and other serious anesthesia and postoperative morbidities such as atelectasis, thromboembolic disease, or stroke. 15 It has been shown that most cases of AUB are due to benign pathology and that the majority are caused by functional disorders. In the current study, 4.2% of the patients required hysterectomy for management of AUB due to failure of medical management or after diagnosis of malignancy noted on endometrial sampling. Medical treatment and other minimally invasive methods, such as endometrial ablation or hysteroscopic myomectomy, can be attempted first in selected cases by the treating gynecologist.16,17 A levonorgestrel intrauterine device has been shown to be a highly effective method for addressing benign cases of AUB, with 87% of patients experiencing relief of menorrhagia after 6 months of treatment. 18 Knowledge of the patient's endometrial histopathology can help avoid overzealous treatment such as hysterectomies and allow successful management of AUB with these conservative modalities. Endometrial sampling offers an outpatient, cost-effective method of directing further management in cases of AUB along with reduction in nonindicated hysterectomies.
Conclusions
The current study showed that the etiology of AUB changes with increasing age and the incidence of premalignant and malignant lesions progressively increase. The importance of endometrial sampling in older women with abnormal bleeding, especially postmenopausal cases, is supported by the current results. In addition, sampling should also be considered in selected younger women, such as those with anovulatory heavy bleeding. This study also emphasizes the possibility of conservative therapy for most cases of abnormal menstrual bleeding.
Footnotes
Author Disclosure Statement
No financial support was received. The authors have no conflicts of interest.