
Abstract
Abstract
Objective:
The aim of this research was to investigate if an association exists between cerclage height (CH) or the ratio of CH-to-cervical length (CL) and delivery prior to 35 weeks gestational age (GA) among patients having undergone cervical cerclage.
Materials and Methods:
A retrospective cohort study was performed examining transvaginal imaging and obstetric medical records data from 106 women who received prenatal care, had a cerclage placed, and delivered at a tertiary referral center in Cincinnati, OH, between July 2012 and December 2014. The primary outcome was delivery prior to 35 weeks gestation.
Results:
No association was found between CH and the rate of preterm birth prior to or after 35 weeks (mean CH: 18.99 mm; standard deviation [SD]: SD 4.71) versus 19.03 mm; SD 6.38; p = 0.97). Additionally, no association was found between the ratio of CH-to-CL and the rate of preterm birth prior to or after 35 weeks (mean ratio: 0.588; SD: 0.174 versus 0.541; SD: 0.170; p = 0.185). The lack of association between both CH and the ratio of CH-to-CL as well as delivery prior to 35 weeks remained when the cohort was stratified by indication for cerclage. The only statistically significant difference was between the ratio of CH-to-CL length in patients who received history-indicated cerclage and delivered prior to or after 28 weeks GA (mean ratio: 0.4969; SD 0.135 versus 0.6479; SD 0.251; p = 0.0166). Otherwise, no association was found when evaluating GA cutoffs of 24, 28, 32, 35, or 37 weeks, or when patients who delivered prior to 28 weeks were compared to patients delivering at or beyond 32 weeks. There was no association between CH nor the ratio of CH-to-CL and latency between cerclage placement and delivery. Six women experienced a very short latency (≤ 3 weeks), and all 6 experienced either an intrauterine fetal demise (n = 3) or neonatal demise (n = 3). Five of these cases (83%) involved placement of a rescue cerclage where the amniotic membrane was exposed and/or prolapsing. The sixth case was performed due to the finding of a 5-mm cervical length on ultrasound imaging with a large U-shaped funnel. In comparing the 6 cases of extremely short latency to the remainder of the cohort with a latency of at least 5 weeks (n = 100), no differences were noted with regard to CH (19 ± 6 mm versus 19 ± 1 mm; p = 0.89) or the ratio of CH-to-CL (0.56 ± 0.13 versus 0.56 ± 0.17; p = 0.93).
Conclusions:
These findings support other reports that have shown no association between CH and GA at delivery. Surgical method (McDonald versus Shirodkar) does not appear to correlate with CH nor GA at delivery, and the factor that bears the strongest correlation with obstetric outcomes remains the indication for the procedure. (J GYNECOL SURG 34:177)
Introduction
G
Management of pregnancy is challenging in a patient who has a history of midtrimester PTDs, a short cervix identified on transvaginal ultrasound (TVUS), or cervical dilation found on a physical examination prior to achieving pregnancy viability. These patients are at increased risk of PTD in the current pregnancy. Cervical cerclage is a proven measure for prevention of preterm birth among at-risk women,3–7 and is associated with increased neonatal survival and decreased morbidity.8,9
It has long been advocated that, in appropriate candidates, placement of the cerclage as cephalad as possible in the cervix is most efficacious. 5 The Shirodkar approach was advocated over the conventional McDonald approach due to the theoretical advantage of higher placement via dissection of the vaginal mucosa off the cervix anteriorly and posteriorly so that the suture could be placed nearer to the internal cervical os. 6 For a patient with a history of trachelectomy or a severely shortened cervix, the abdominal approach to cervical cerclage is advocated—again to allow for the most cephalad placement of the suture. 10 Some surgeons have even attempted to place a second suture at the time of the procedure with hopes of optimizing cerclage height (CH) and obstetric outcomes.11,12 However, studies have failed to demonstrate improvement in obstetric outcomes with this second suture. This and other accounts have raised suspicion that the time-honored belief that “higher is better” might not be true when it comes to cervical cerclage.
The objective of this study was to investigate if CH (as determined by the sonographic measurement of the distance from the cross-sectional cerclage diameter to the external os) or the ratio of the CH to the total cervical length (CL) are associated with PTD prior to 35 weeks gestation.
Materials and Methods
The records of all women having received history-, ultrasound (US)–, or examination-indicated cerclages between July 2012 and December 2014, at the current authors' tertiary-care center, comprised of two large community hospitals in Cincinnati, OH, were evaluated for inclusion in the current analysis. This timeframe was chosen, as it coincided with implementation of a new electronic records system at the authors' institution. Institutional review board approval was granted on October 8, 2014, and due to the nature of the study, consent requirement was waived.
Current Procedural Terminology (CPT) coding was utilized to identify subjects. Data were collected from the electronic medical records to determine eligibility among women receiving care from the obstetrics/gynecology-resident or maternal–fetal medicine (MFM)–practices. Subjects were excluded for age <18 years, multiple gestations, transabdominal cerclage, or if delivery occurred at an outside hospital. Subjects' obstetric dating was calculated by last menstrual period if it was consistent with the first obstetrical US; otherwise, dating was determined by findings on first obstetric US imaging. 13
History-indicated cerclage was defined as one placed between 110/7 and 236/7 weeks gestation due to a history of one or more second-trimester losses related to painless cervical dilation, in the absence of labor or placental abruption, or for a history of prior cerclage placement. An ultrasound-indicated cerclage was defined as one placed between 110/7 and 236/7 weeks gestation due to the TVUS finding of a CL measurement <25 mm in conjunction with additional risk factors. Finally, an examination-indicated cerclage was defined as one placed between 110/7 and 236/7 weeks of gestation based on the finding of cervical dilation of at least 1 cm on visual inspection or digital examination in the absence of active labor or clinical infection noted on amniocentesis.
The primary outcome of interest was PTD prior to 35 weeks gestation. Secondary outcomes included GA at delivery, indication for nonspontaneous delivery, staffing physician, surgical technique, latency until first US, and cerclage indication. Demographic information was collected, including age, body mass index, gravidity, race, history of preterm birth, history of conization or loop electrosurgical excision procedure, and GA at time of cerclage placement. Primary comparisons were made between the CH and the ratio of the CH to the total CL with respect to pregnancy outcomes.
Given the retrospective nature of this investigation, all stored TVUS images obtained during the clinical care for each participant were reviewed for potential inclusion. Imaging was performed by American Institute of Ultrasound in Medicine–certified obstetric sonographers using a standard technique. 14 At least 3 images were evaluated for measurement in each subject by a single researcher who was blinded to outcome data. All study-related measurements were performed using postprocessing software on the stored images—after the participant had delivered such that these measurements did not affect clinical care.
First, a straight line was drawn between the external and internal os, and the shortest of the three measurements was recorded as the CL. Only straight-line measurements of the CL were performed in accordance with the protocol established by Kushnir et al. 14 Then, a straight line was drawn between the cross-sectional image of the suture in the anterior and posterior cervix; the distance between this level along the cervical canal and the external os was recorded as the CH, as previously described (Fig. 1). 15 When this line representing the cross-sectional diameter of the cerclage was not found to be exactly perpendicular to the cervical canal, the point where the line intersected the cervical canal was used to denote the height. The distance above the cerclage is accounted for in the CH-to-CL length ratio. These measurements were performed on the first postoperative TVUS.
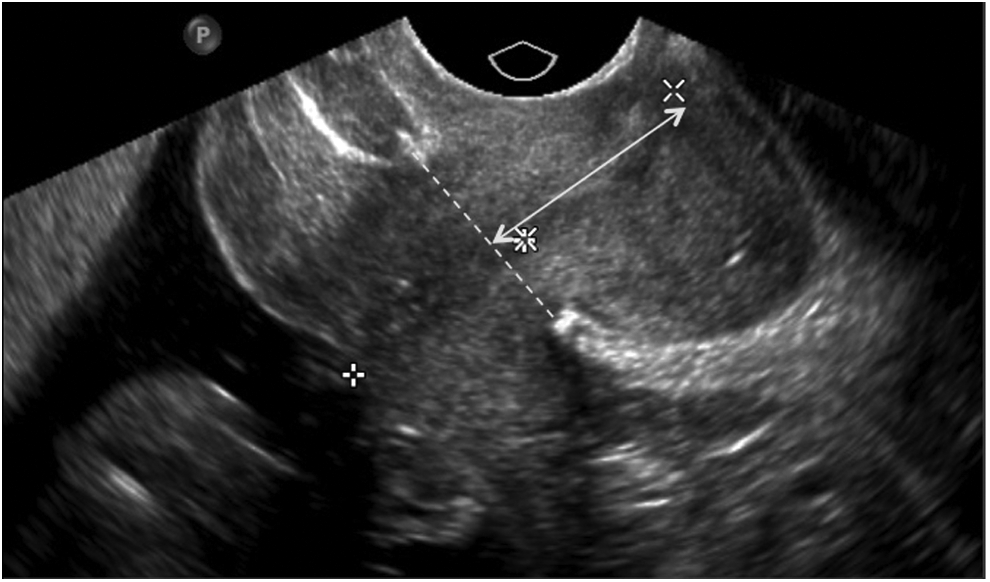
Illustration of the cerclage height measurement.
All analyses were performed using SPSS, version 16 (IBM Corporation, Armonk, NY). Data are presented as proportions and means, and comparisons were made with the χ2 or Fisher's exact tests among categorical variables when appropriate. The t-test or Mann–Whitney-U tests were performed on continuous variables when appropriate, and p-values <0.05 were considered to be statistically significant.
Results
One hundred and six women were identified as meeting inclusion criteria. Sixty women (57%) received history-indicated cerclage, 27 women (25%) received US-indicated cerclage, and 19 women (18%) received examination-indicated cerclage. The demographic characteristics were similar among the subjects (Table 1).
Data presented as mean (standard deviation).
Data presented as median (range).
Data presented as n (%).
BMI, body mass index; PTD, preterm delivery; LEEP, loop electrosurgical excision procedure; GA, gestational age.
The median GA at delivery was 37.1 weeks GA (range: 17.4–41.3). The median latency between cerclage placement and the first postoperative TVUS was 10 days (range: 0–48). An MFM attending supervised the cerclage placement for 72% (76/106) of the subjects; the remainder of the patients had cerclages placed by a resident under the supervision of generalist obstetrics/gynecology staff member. Eighty-six of the 106 (81%) patients had received McDonald cerclages, with the remainder receiving Shirodkar cerclages (Table 2).
Bold italic values indicate significance.
Data presented as mean (standard deviation).
Data presented as median (range).
Data presented as n (%).
GA, gestational age; US, ultrasound; MFM, Maternal–Fetal Medicine.
The data for CH and the ratio of CH-to-CL were found to be normally distributed. There was no significant difference between the CH in patients who delivered prior to 35 weeks gestation (19.03 mm; standard deviation [SD]: 6.382) versus delivery after 35 weeks (18.99 mm; SD: 4.704; p = 0.97). Furthermore, the ratio of CH-to-CL did not differ between the 2 groups (0.5879; SD: 0.172 versus 0.5414; SD; 0.167; p = 0.18). This held true among the entire population and among subgroups stratified by cerclage indications. Surgical technique was not associated with a difference in CH nor the ratio of CH-to-CL and delivery before 35 weeks (Table 3).
Data presented as mean (standard deviation).
Data presented as n (%).
CH, cerclage height; CL, cerclage length; US, ultrasound.
There was no significant difference between either CH (Fig. 2) or the ratio of CH-to-CL (Fig. 3) and GA at delivery. The only statistically significant difference was between the ratio of CH-to-CL in patients who received history-indicated cerclages and delivered prior to or after 28 weeks; GA (mean ratio: 0.4969; SD 0.135 versus 0.6479; SD 0.251; p = 0.0166). Otherwise, with respect to both CH and the ratio of CH-to-CL, there was no difference when evaluating GA cutoffs of 24, 28, 32, 35, or 37 weeks, or when patients who delivered prior to 28 weeks were compared to patients delivering at or beyond 32 weeks.
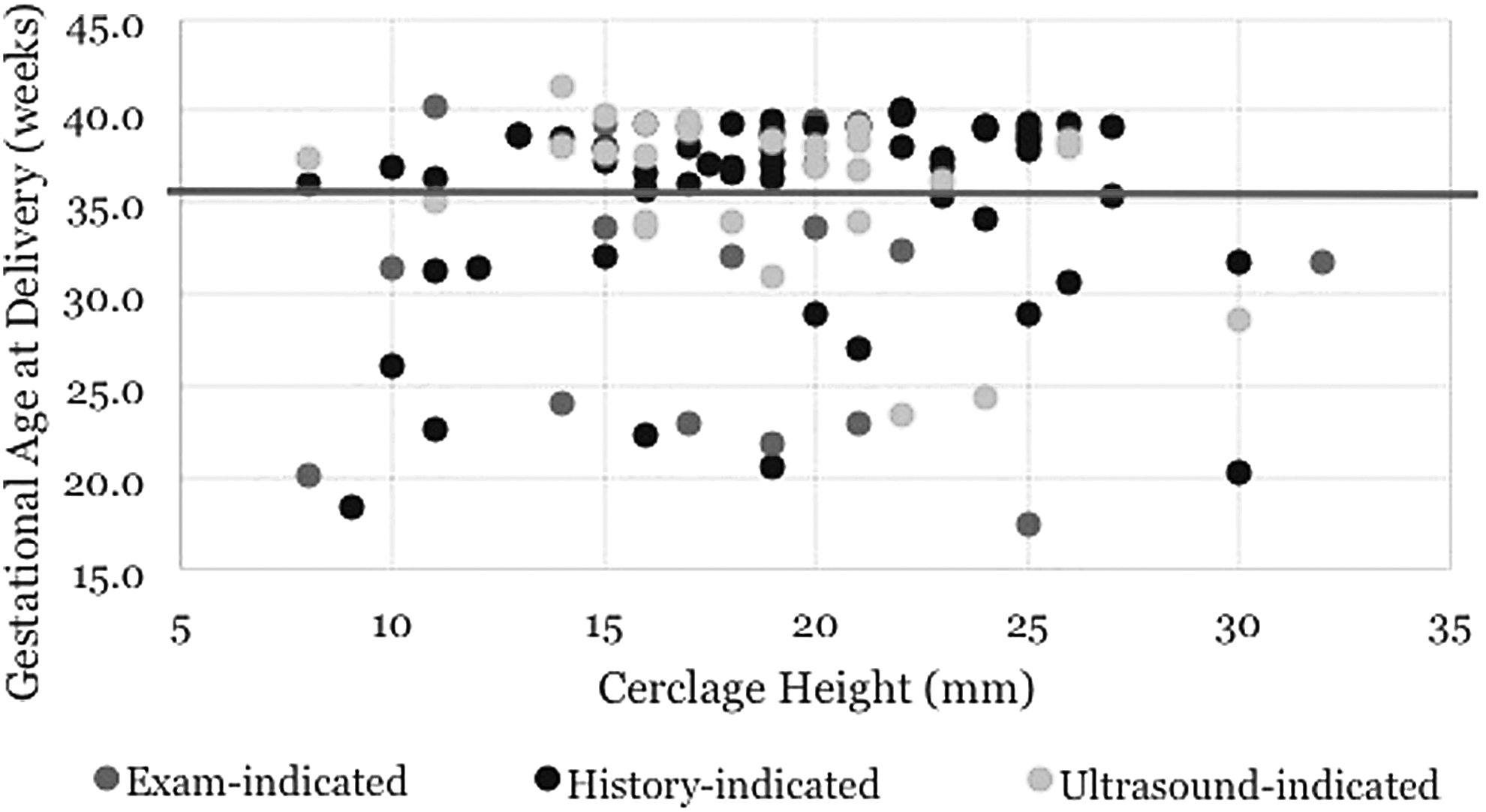
The association of cerclage height and gestational age at delivery.

The association of the ratio of cerclage height (CH) to cervical length (CL) and gestational age at delivery.
The median latency period between cerclage placement and delivery for the entire cohort was 137.5 (range: 2–205) days. Ninety-four percent had a latency of at least 28 days, and 90% had a latency period of 56 days or more. There was no association between CH nor the ratio of CH-to-CL and latency between cerclage placement and delivery. Six women experienced very short latency (≤ 3 weeks), and all 6 women experienced either an intrauterine fetal demise (IUFD; n = 3) or neonatal demise (n = 3). Five of these cases (83%) involved placement of a rescue cerclage where the amniotic membrane was exposed and/or prolapsing. The sixth case was performed due to the finding of a 5-mm cervical length on US imaging with a large U-shaped funnel. In comparing the 6 cases of extremely short latency to the remainder of the cohort with a latency of ≥5 weeks (n = 100), no differences were noted with regard to CH (19 ± 6 mm versus 19 ± 1 mm; p = 0.89) or the ratio of CH-to-CL (0.56 ± 0.13 versus 0.56 ± 0.17; p = 0.93).
The rate of preterm birth under 35 weeks gestation was 33% among the entire cohort, with a spontaneous preterm birth rate secondary to preterm labor under 35 weeks of only 13% (Table 4). The rate of nonspontaneous preterm birth <35 weeks of gestation was 26% (5/19) in the examination-indicated cerclage group, 22% (6/27) in the US-indicated group, and 17% (10/60) in the history-indicated group. An additional 4 patients were delivered between 35 and 37 weeks, for a total of 25 patients (24%) delivered prior to 37 weeks gestation for obstetrical or fetal indications, including chorioamnionitis (52%), preterm premature rupture of membranes (PPROM; 32%), preeclampsia (8%), IUFD (4%), or history of classical cesarean section (4%). See Table 4. Finally, the presence of funneling or debris on postoperative US was not associated with delivery before 35 weeks gestation regardless of cerclage indication (37% versus 38%; p = 0.93).
Data presented as median (range).
Data presented as n (%).
US, ultrasound; PTD, preterm delivery; GA, gestational age. IUFD, intrauterine fetal demise; NND, neonatal demise; PPROM, preterm premature rupture of membranes.
Discussion
The aim of this research was to evaluate the association between CH and pregnancy outcomes, and these findings challenge the axiom introduced by McDonald and perpetuated for decades, that the cerclage suture be placed “as high as possible” within the cervix. 5 The incorporation of TVUS into modern-day obstetrics allows for the ability to quantify this effort and investigate CH with obstetric outcomes. This retrospective cohort investigation failed to demonstrate an association between CH and GA at delivery, nor between the ratio of CH-to-CL and GA at delivery, regardless of indication for cerclage. While an 18-mm threshold of CH was identified as bearing an association with lowered rates of preterm birth in a US-indicated cerclage population, 15 the current authors did not find a similar association. The current study population was comprised of a majority of women having undergone history-indicated cerclage, and the findings support the lack of association previously reported in the history-indicated cerclage literature.16,17 To the current authors' knowledge, this is the first evaluation of CH or the ratio between CH-to-CL among women having undergone examination-indicated or “rescue” cerclage, and it appears that CH might not bear an association with obstetric outcomes among this population as well.
A significant strength of the current study was the evaluation of a large cohort of women who had transvaginal cerclage placed for history, US, and examination-indications. The availability of high-quality postsurgical sonographic imaging for all of the subjects is unique and allowed for methodologically sound CH measurement. The investigator who performed postproduction measurements of the CH and CL was blinded to the pregnancy outcomes of the cohort.
There were several limitations to the current study. Patients were not excluded from the study for indicated PTDs, whereas this population had been excluded in previously reported studies investigating CH.15,16 Twenty-five patients appeared to have been induced or delivered via cesarean section prior to 37 weeks gestation for obstetrical or fetal indications, including chorioamnionitis, PPROM, preeclampsia, IUFD, or history of classical cesarean section. Given the retrospective nature of the analysis, it was often difficult to determine the exact indication for delivery such that participants were not excluded based on this factor. Finally, the modest number of women with US- or examination-indicated cerclages limited robust comparisons within or between these subgroups.
Postoperative imaging utilizing TVUS following cerclage placement remains controversial. Various recommendations have been made regarding whether or not to perform postoperative imaging, the optimal timing for this, 18 and certain sonographic findings that could portend a poor prognosis. 19 None of the current findings can lend strong support to this practice. While the current authors reported information on the CH-to-CL ratio to account for the cervix proximal to the suture, some researchers have commented on the association of the absence of any proximal cervix and preterm birth when evaluated in the late second trimester. 20 It is clear that more research is needed to clarify the role for, optimal timing of, and anatomical points of interest in studying postsurgical cerclage imaging.
Conclusions
The height of cervical cerclage placement does not appear to directly correlate with preterm birth reduction or GA at delivery. Surgical method (McDonald versus Shirodkar) does not appear to correlate with CH nor GA at delivery, and the factor that bears the strongest correlation with obstetric outcomes remains the indication for the procedure.
Footnotes
Author Disclosure Statement
None of the authors declare any financial or personal conflicts of interest to disclose.